
Garden of Life
Dr. Formulated DHA 1g by Garden of Life
30 softgels · 30-day supply
High-Potency DHA for Brain, Eye, and Heart Health$31.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Soy Free·Dairy Free·Peanut Free·Crustacean Shellfish Free·Preservative Free·Artificial Color Free·
Garden of Life Dr. Formulated DHA 1g overview
If you rarely eat seafood and want a direct brain and eye dose, DHA 1000 mg is a targeted pick. It fits adults with a low Omega-3 Index who want to raise it within 4 to 12 weeks, and those planning pregnancy but not eating fish. This is also useful if your focus is cognition or visual performance rather than triglyceride lowering. If your triglycerides are elevated, EPA-heavy omega-3 (often 2–4 g/day of EPA+DHA) works better than DHA alone.
DHA is the omega-3 your brain and retina build into cell membranes, which improves membrane fluidity and signal transmission at synapses. It also gives rise to resolvins and protectins (short-lived signaling molecules that help turn off inflammation), which is why some people see small drops in hs-CRP (a blood marker of inflammation). This softgel uses triglyceride-form omega-3, which absorbs well when taken with food, and includes 75 mg DPA, a related omega-3 that can convert to DHA or EPA as needed.
Take one softgel daily with a meal that contains fat; absorption is better than on an empty stomach. Expect your Omega-3 Index to rise over 1 to 3 months, then re-test to see if one daily softgel is enough for maintenance. If you also want triglyceride reduction, consider adding EPA or switching to a higher EPA:DHA fish oil under clinician guidance. Plant-based? An algal DHA 1,000 mg can serve a similar role.
Fish allergy is a hard stop for fish oil; choose algal DHA instead. If your LDL cholesterol tends to run high, know that DHA can nudge LDL up in some people; check a lipid panel after 8 to 12 weeks. On prescription blood thinners like warfarin or direct-acting oral anticoagulants, discuss dosing with your clinician. For surgery, many surgeons ask patients to pause omega-3 one week prior.
Wondering whether EPA or DHA is better? EPA is the workhorse for lowering triglycerides on a lipid panel, while DHA is the structural omega-3 for brain and retina membranes. If cognition, vision, or pregnancy planning is your priority, DHA-forward makes sense. Garden of Life’s Dr. Formulated DHA 1g delivers that focus without a large EPA load.
Frequently asked questions
Is DHA or EPA better for high triglycerides?
EPA is better for lowering triglycerides. Most responders need 2–4 grams per day of combined EPA+DHA, usually EPA-heavy. A DHA-only 1,000 mg softgel is aimed more at brain and eye tissue repletion than triglyceride reduction.
How long does DHA 1000 mg take to work?
For blood levels, expect your Omega-3 Index to rise within 4–12 weeks. Cognitive or visual benefits are slower and more subtle, tracking with membrane turnover. Re-test after 1–3 months to see if the dose is adequate or needs adjusting.
Does DHA raise LDL cholesterol?
It can in some people. DHA sometimes nudges LDL cholesterol up slightly while often improving LDL particle size. If LDL is a concern, re-check a lipid panel after 8–12 weeks or consider shifting toward EPA-predominant omega-3.
Can I take DHA with blood thinners?
Use caution. Omega-3s can modestly reduce platelet stickiness. If you’re on warfarin or a direct-acting oral anticoagulant, talk with your prescriber and avoid making large, unmonitored dose changes.
Should I take DHA with food or on an empty stomach?
Take it with a meal that contains fat. Triglyceride-form omega-3 absorbs better with dietary fat and is less likely to cause fishy burps or reflux compared with taking it on an empty stomach.
Is DHA safe in pregnancy?
DHA is commonly used in pregnancy to cover low seafood intake, but use a prenatal-safe brand and confirm dose with your obstetric clinician. If you avoid fish, choose algal DHA to eliminate fish allergen concerns.
What side effects should I expect with DHA?
Most people tolerate it well. Possible issues include fishy aftertaste, mild reflux, or loose stools, usually reduced by taking with food. Rarely, bruising can increase at high omega-3 intakes, especially with anticoagulants.
How to take it & ingredients
Suggested use: Adults take 1 softgel daily with food. Not intended for children.
Active ingredients
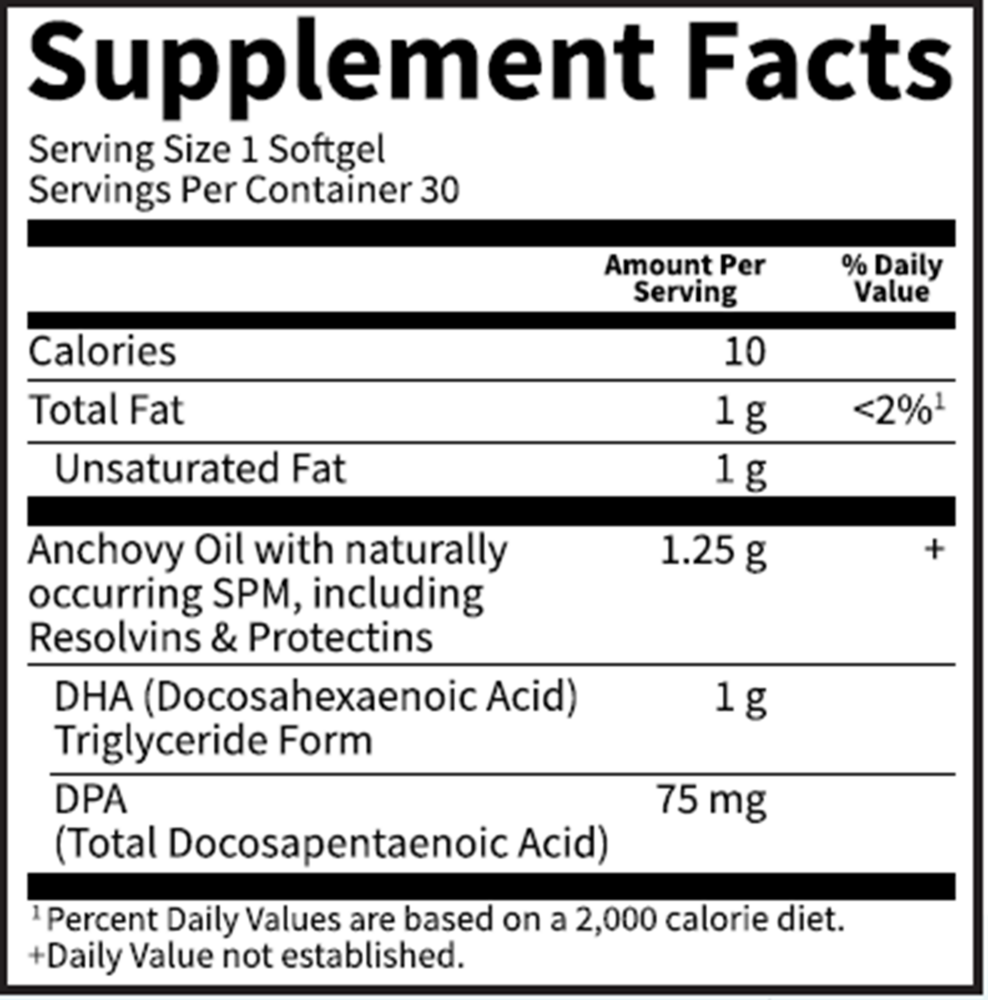
1 softgel per serving · 30 servings
Docosahexaenoic Acid
DHA (Triglyceride Form)
DHA (Triglyceride Form)
1000 mg
Docosapentaenoic Acid
DPA
DPA
75 mg
Other ingredients: Non-GMO PlantGel™ Softgel, Non-GMO Lemon Flavor, Non-GMO Rosemary Extract
Certifications
Benefits
Warnings
Customers also considered

Thorne
Advanced DHA
60 gelcaps
$30.00extra 10% off with Subscribe & Save

Garden of Life
Dr. Formulated Advanced Omega
60 softgels
$31.99extra 19% off with Subscribe & Save
Garden of Life
Dr. Formulated Prenatal DHA
30 softgels
$29.99extra 20% off with Subscribe & Save

Pure Encapsulations
EPA/DHA Essentials
90 softgels
$41.50extra 21% off with Subscribe & Save