
Nature's Way
Fisol Fish Oil 250 mg by Nature's Way
180 softgels · 180-day supply
Supports Heart Health with Essential Omega-3 Fatty Acids$37.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Dairy Free·Wheat Free·Yeast Free·Artificial Color Free
Nature's Way Fisol Fish Oil overview
If you want enteric coated fish oil to avoid fishy burps and keep a steady maintenance intake, this fits. It’s a light dose of omega-3 (EPA and DHA) for people who eat little seafood, have an Omega-3 Index in the lower normal range, or are pregnancy planning but not eating fish. If your triglycerides are elevated or you’re targeting joint flare-ups, this amount is usually too low to move labs on its own.
EPA and DHA reduce how much fat your liver pushes out as VLDL particles (the triglyceride-carrying packages on a lipid panel) and nudge cells to burn fatty acids for energy. Many responders see triglycerides come down within 4–12 weeks at higher, gram-level intakes. These fats also shift membrane signaling toward fewer pro-inflammatory eicosanoids (short-lived messengers), which is why hs-CRP (a blood inflammation marker) sometimes falls. The enteric coating releases fish oil in the intestine, which improves comfort and cuts reflux-related burps.
Take one softgel up to three times daily with water, ideally with meals to aid absorption and reduce aftertaste. If your goal is a healthier Omega-3 Index, recheck it in 8–12 weeks and adjust. For triglyceride reduction, most adults need gram-level EPA+DHA from concentrated fish oil or prescription icosapent ethyl, not a maintenance micro-dose like this.
Use caution if you’re on anticoagulants (drugs that reduce blood clotting) such as warfarin, apixaban, or clopidogrel, or if you have surgery scheduled—discuss dosing with your clinician. People with a fish or shellfish allergy should avoid fish oil. If you’ve had atrial fibrillation (an irregular heartbeat), stay within moderate doses and get cardiology input, since very high omega-3 intakes have been linked to recurrence in some studies.
Is krill oil better? It’s pricier per mg of EPA+DHA and hasn’t outperformed fish oil in head-to-head triglyceride data. What about immune benefits? Outside frank deficiency, effects are modest; use labs like Omega-3 Index and hs-CRP to guide whether it’s doing anything meaningful for you.
Frequently asked questions
Is 250 mg of omega-3 enough if I don’t eat fish?
It’s a maintenance dose, not repletion. If your Omega-3 Index is low, you’ll usually need a higher daily total (often 1,000 mg+ EPA+DHA) for 8–12 weeks, then step down.
Does fish oil lower triglycerides and how long does it take?
At gram-level EPA+DHA, triglycerides often drop within 4–12 weeks. A 250 mg dose is unlikely to change a lipid panel; consider a higher-concentration fish oil or prescription-grade.
Does fish oil thin your blood?
It has mild antiplatelet effects. Bleeding risk is low at typical doses, but if you take warfarin, apixaban, rivaroxaban, or clopidogrel, speak with your clinician before starting.
Can I take fish oil on an empty stomach?
You can, but taking it with meals improves absorption and reduces reflux. Enteric-coated fish oil further cuts fishy burps by releasing in the intestine.
Are fish oil burps normal and how do I prevent them?
They’re common with non-coated oils. Enteric-coated softgels, taking with food, and splitting doses across the day usually solve it.
Is fish oil safe in pregnancy?
Moderate-dose EPA/DHA is generally considered safe and useful if you don’t eat fish. Choose a product tested for contaminants and coordinate dosing with your obstetric clinician.
Fish oil vs krill oil: which should I pick?
Pick based on EPA+DHA per dollar and lab goals. Fish oil usually delivers more EPA+DHA for cost and has stronger data for triglycerides than krill oil.
How will I know it’s working?
Re-test your Omega-3 Index after 8–12 weeks. If you’re targeting triglycerides, repeat a fasting lipid panel; look for changes alongside habits like diet and activity.
How to take it & ingredients
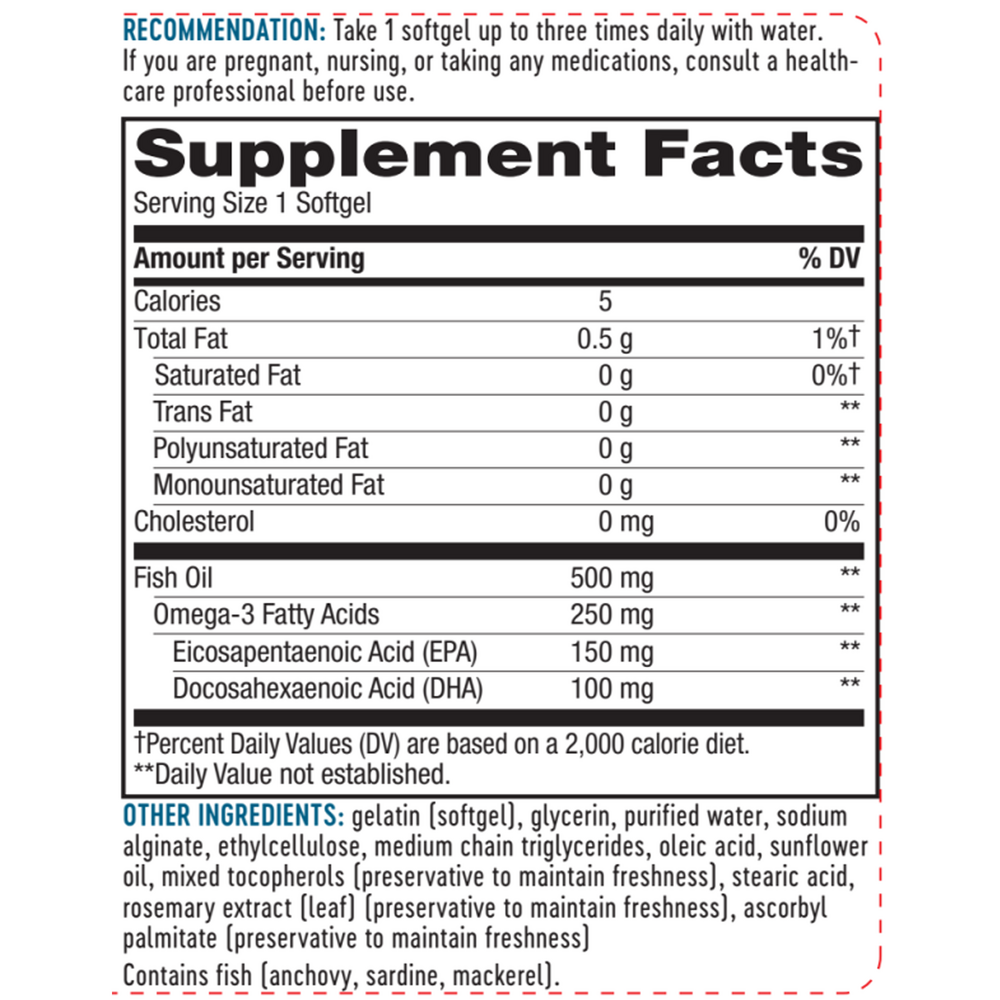
Suggested use: Take one softgel up to three times daily with water.
Active ingredients
1 softgel per serving · 180 servings
▼
Omega-3 Fatty Acids
250 mg
EPA
Eicosapentaenoic acid
Eicosapentaenoic acid
150 mg
DHA
Docosahexaenoic acid
Docosahexaenoic acid
100 mg
Other ingredients: Gelatin (softgel), Glycerin, Purified water, Sodium alginate, Ethylcellulose, Mixed tocopherols (preservative to maintain freshness), Medium chain triglycerides, Oleic acid, Sunflower oil, Stearic acid, Rosemary (leaf) extract (preservative to maintain freshness), Ascorbyl palmitate (preservative to maintain freshness)
Certifications
Benefits
Warnings
Customers also considered

Thorne
Advanced DHA
60 gelcaps
$30.00extra 10% off with Subscribe & Save

Garden of Life
Dr. Formulated Advanced Omega
60 softgels
$31.99extra 19% off with Subscribe & Save
Garden of Life
Dr. Formulated DHA 1g
30 softgels
$31.99extra 19% off with Subscribe & Save
Garden of Life
Dr. Formulated Prenatal DHA
30 softgels
$29.99extra 20% off with Subscribe & Save