

Nature’s Way
Alive! Men’s 50+ Ultra Potency by Nature’s Way
60 tablets · 60-day supply
Comprehensive Nutritional Support for Men Over 50$XX.XX$29.99retail
Purchase option
20% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Gluten Free·Artificial Color Free
Nature’s Way Alive! Men’s 50+ Ultra Potency overview
If you’re a man over 50 looking for a one‑a‑day multivitamin for men over 50, this fits when your diet or labs suggest gaps. It’s useful if your Vitamin D, 25-Hydroxy is in the lower range, if you eat little seafood or organ meats (B12, selenium, zinc), or if metformin or acid‑suppressing meds have nudged your Vitamin B12 down or homocysteine (an amino acid tied to B-vitamin status) up. The dose here is maintenance‑leaning: good for steady coverage, not for treating established deficiency without clinician guidance.
You get vitamin D3 (the form your skin makes) at 2,000 IU, which typically nudges Vitamin D, 25-Hydroxy upward within 4–12 weeks. Methylcobalamin B12 (a bioactive B12 form) and folic acid help keep homocysteine in check, which matters for vascular health. The blend splits vitamin A between beta‑carotene (plant precursor) and retinyl acetate (preformed A), balancing safety and immediate activity. Minerals lean on carbonate/oxide salts; they’re fine for a multivitamin but not ideal if you’re specifically repleting magnesium. Small adds like CoQ10, ginkgo, rhodiola, and saw palmetto are present, but at modest amounts that serve as extras, not stand‑alone doses.
Take one tablet daily with food, ideally breakfast or lunch. Food improves absorption of fat‑soluble vitamins A, D, E, and K and tames any stomach upset from mineral salts. Because the B‑vitamins are high‑potency and mildly stimulating for some, earlier in the day is better than evening. Don’t stack this with other multis. If your Vitamin D, 25-Hydroxy is low, you may need a separate D3 repletion plan first, then this for maintenance.
If you take warfarin (a blood thinner), the vitamin K here can interfere with dosing—use a K‑consistent plan only under your prescriber’s guidance. If you have a history of high selenium intake (Brazil nuts or separate selenium), note this has 200 mcg, which is near the top of daily needs; don’t add more. Thyroid disease warrants a quick check with your clinician before extra iodine. Saw palmetto can slightly lower PSA (the prostate blood test), so tell your doctor you’re taking it during screening.
Will you feel an energy boost? If you were low on B‑vitamins or D, many notice steadier energy in 1–3 weeks; lab shifts typically show in 4–12 weeks. Is folic acid OK? Yes for most; if you’ve been told you have an MTHFR variant or have high homocysteine, consider checking Folate and homocysteine and discuss methylfolate with your clinician. Can you pair this with magnesium? Yes, but choose a better‑absorbed form like magnesium glycinate at a separate time.
Frequently asked questions
Do men over 50 really need a multivitamin?
Not everyone. If your diet is consistent and labs look good, you may not need one. It’s practical coverage if Vitamin D, 25-Hydroxy or Vitamin B12 runs low, appetite is smaller, or meds like metformin or PPIs reduce B12 absorption.
When is the best time to take a men’s 50+ multivitamin?
Take it with a meal, preferably breakfast or lunch. Food improves absorption of vitamins A, D, E, and K and reduces stomach upset. Morning also avoids sleep interference from high‑potency B‑vitamins in sensitive people.
Is this multivitamin safe with blood thinners?
If you’re on warfarin, be cautious. The vitamin K can alter your dose requirements. Don’t start or stop without your prescriber; keep intake consistent and monitor INR closely. Direct oral anticoagulants aren’t vitamin‑K dependent.
How long until this multivitamin affects my labs?
Most see Vitamin D, 25-Hydroxy, B12, and folate changes within 4–12 weeks. Retest after 8–12 weeks to judge effect, then adjust. Energy changes, if you were low, often appear in 1–3 weeks.
Does saw palmetto in this help the prostate?
The dose here is small, so don’t expect symptom relief on its own. Evidence for urinary symptom improvement is mixed even at higher doses. It can slightly lower PSA, so inform your clinician during screening.
Is methylcobalamin better than cyanocobalamin for B12?
Both raise B12. Methylcobalamin is a bioactive form and is fine to use; cyanocobalamin has the most stability data. If your Vitamin B12 is low, the form matters less than taking an adequate dose and retesting.
Can I take calcium or magnesium with this multivitamin?
Yes, but space them out if you use thyroid meds or certain antibiotics. For magnesium repletion, pick glycinate or citrate at another time of day; the magnesium oxide in multis is modest and less well absorbed.
Will the ginkgo or ginseng thin my blood?
At the small amounts in this blend, major effects are unlikely, but ginkgo can increase bleed risk when combined with anticoagulants or antiplatelets. If you use those drugs, review the full formula with your clinician.
How to take it & ingredients
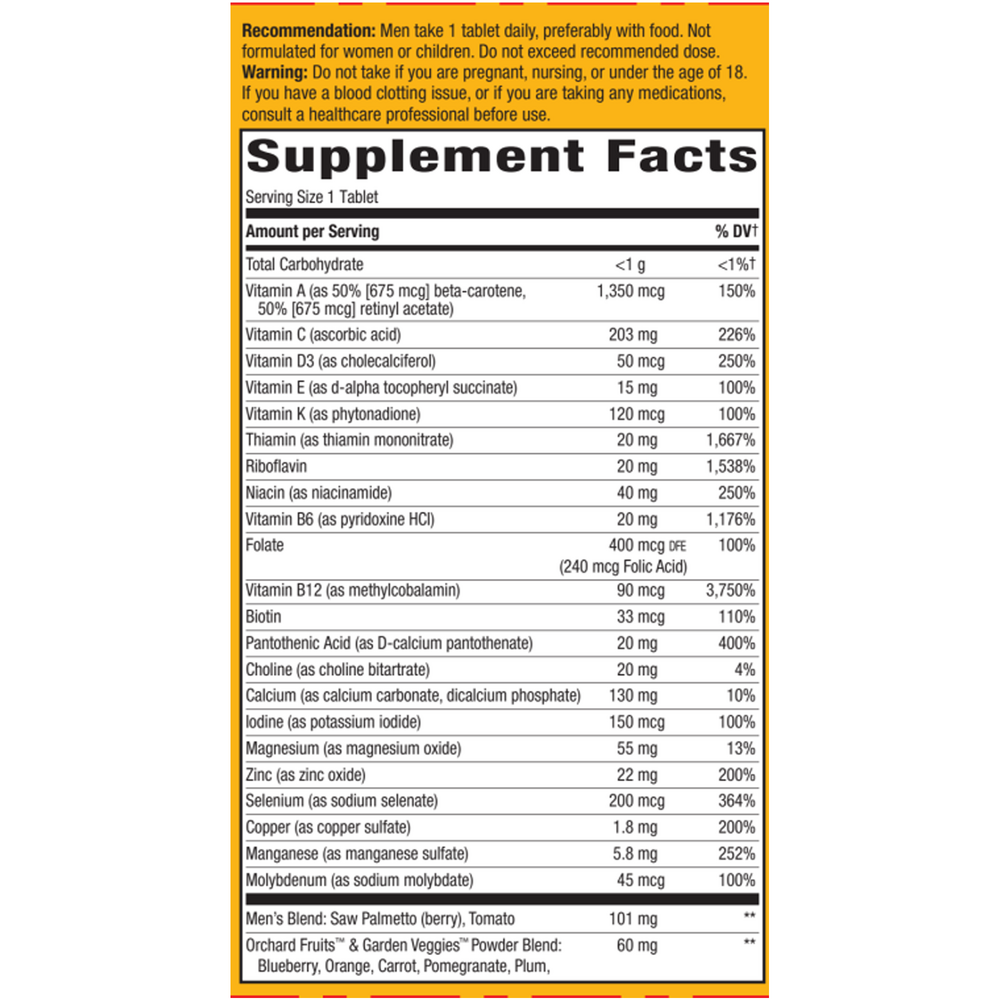
Suggested use: Men take 1 tablet daily, preferably with food. Not formulated for women or children. Do not exceed recommended dose.
Active ingredients
1 tablet per serving · 60 servings
Vitamin A
50% beta-carotene, 50% retinyl acetate
50% beta-carotene, 50% retinyl acetate
3375.45 IU, 1350 mcg
Vitamin C
Ascorbic acid
Ascorbic acid
203 mg
Vitamin D3
Cholecalciferol
Cholecalciferol
2000 IU, 50 mcg
Vitamin E
D-alpha tocopheryl succinate
D-alpha tocopheryl succinate
13.5 IU, 15 mg
Vitamin K
Phytonadione
Phytonadione
120 mcg
Thiamine
Thiamine mononitrate
Thiamine mononitrate
20 mg
Riboflavin
20 mg
Niacin
Niacinamide
Niacinamide
40 mg
Vitamin B6
Pyridoxine HCl
Pyridoxine HCl
20 mg
Folate
Folic acid
Folic acid
400 mcg DFE, 240 mcg
Vitamin B12
Methylcobalamin
Methylcobalamin
90 mcg
Biotin
33 mcg
Pantothenic Acid
D-calcium pantothenate
D-calcium pantothenate
20 mg
Choline
Choline bitartrate
Choline bitartrate
20 mg
Calcium
Calcium carbonate, dicalcium phosphate
Calcium carbonate, dicalcium phosphate
130 mg
Iodine
Potassium iodide
Potassium iodide
150 mcg
Magnesium
Magnesium oxide
Magnesium oxide
55 mg
Zinc
Zinc oxide
Zinc oxide
22 mg
Selenium
Sodium selenate
Sodium selenate
200 mcg
Copper
Copper sulfate
Copper sulfate
1800 mcg
Manganese
Manganese sulfate
Manganese sulfate
5.8 mg
Molybdenum
Sodium molybdate
Sodium molybdate
45 mcg
Men’s Blend
Saw Palmetto (berry), Tomato
Saw Palmetto (berry), Tomato
101 mg
Orchard Fruits™ & Garden Veggies™ Powder Blend
Blend of 26 fruits and vegetables
Blend of 26 fruits and vegetables
60 mg
Mind & Body Energy Blend
Asian ginseng extract, eleuthero, ginkgo biloba extract, gotu kola, rhodiola extract
Asian ginseng extract, eleuthero, ginkgo biloba extract, gotu kola, rhodiola extract
30 mg
Cardio Blend
Hawthorn berry, Japanese knotweed extract, coenzyme Q10
Hawthorn berry, Japanese knotweed extract, coenzyme Q10
20 mg
Citrus Bioflavonoid Complex
From orange, grapefruit, lemon, lime, tangerine
From orange, grapefruit, lemon, lime, tangerine
20 mg
Daily Greens™ Blend
Spirulina, kelp, barley grass, chlorella, blue-green algae, and other botanicals
Spirulina, kelp, barley grass, chlorella, blue-green algae, and other botanicals
20 mg
Inositol
20 mg
Mushroom Mycelial & Primordia Biomass Defense Blend
Organic reishi, shiitake, maitake, chaga, and other mushrooms
Organic reishi, shiitake, maitake, chaga, and other mushrooms
20 mg
Digestive Enzyme Blend
Betaine HCl, bromelain, papain
Betaine HCl, bromelain, papain
7 mg
Rutin
From Sophora japonica flower bud extract
From Sophora japonica flower bud extract
5 mg
Lutein
From Aztec marigold flower extract
From Aztec marigold flower extract
1 mg
Other ingredients: Cellulose, Stearic acid, Sodium croscarmellose, Silica, Magnesium stearate, Hypromellose, Gelatin, Glycerin, Brown rice
Certifications
Benefits
Warnings
Customers also considered

Thorne
Advanced Nutrients
240 capsules
$72.00
Add to cart for lower price

Ortho Molecular Products
Alpha Base® Capsules with Iron
240 capsules
$74.31
Add to cart for lower price

Ortho Molecular Products
Alpha Base® Capsules without Iron
120 capsules
$46.79
Add to cart for lower price
Ortho Molecular Products
Alpha Base® Premier Packs
30 packets
$109.50
Add to cart for lower price