

Ortho Molecular Products
Alpha Base® Capsules without Iron by Ortho Molecular Products
120 capsules · 30-day supply
Comprehensive Multivitamin Blend for Optimal Daily Nutritional Support$46.79
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Alpha Base® Capsules without Iron overview
If your Ferritin (the blood marker of iron stores) runs high, you’re a man or a post‑menopausal woman, or you get constipated with iron, a multivitamin without iron is the right lane. This formula suits adults who want comprehensive coverage without extra iron, and who plan to track Vitamin D, 25-Hydroxy and Homocysteine if they’re tuning dose. If you’re menstruating and your Ferritin is low, choose a multi with iron or add iron separately.
Methylcobalamin (active B12) and Quatrefolic 5‑MTHF (the bioactive folate) bypass common genetic bottlenecks and can lower Homocysteine (a methylation byproduct tied to vascular risk) within 4–8 weeks in responders. Chelated minerals like magnesium glycinate/lysinate and zinc bisglycinate are gentle on the gut and better absorbed than oxides. Vitamin K2 MK‑7 (the long‑acting form) complements K1 for bone and vascular calcium handling, while mixed tocopherols round out vitamin E beyond plain alpha‑tocopherol.
Take 4 capsules daily with food. Most patients do best splitting the dose, 2 with breakfast and 2 with dinner, to improve absorption and reduce nausea. The 25 mcg (1,000 IU) of vitamin D3 is a maintenance dose; if your Vitamin D, 25-Hydroxy is low, you’ll likely need higher D3 short term under clinician guidance, then step down and let the multi maintain.
Vitamin K1/K2 interfere with warfarin, so skip this if your dose is managed on that drug. Separate thyroid hormone (levothyroxine) by 4 hours from minerals like calcium, magnesium, and zinc. Magnesium and zinc bind certain antibiotics (tetracyclines, quinolones), so dose those 2–6 hours apart. Chromium can modestly lower glucose; monitor if you use insulin or sulfonylureas. Thyroid disease? Extra iodine warrants clinician input.
If your Ferritin is low or you have heavy periods, an iron‑containing multi is usually more appropriate. Pregnancy or trying to conceive calls for a prenatal with lower preformed vitamin A and tailored choline and iodine. If you’ve had prior B6‑related neuropathy, avoid high‑B6 complexes and get your B6 level checked, since this formula is higher than a basic RDA‑level multi.
Frequently asked questions
Is a multivitamin without iron OK for women?
Yes for many, especially post‑menopausal women or those with normal to high Ferritin. If you menstruate and your Ferritin is low or you feel fatigue from iron deficiency, use a multi with iron or add an iron supplement under guidance.
Do I take this multivitamin with food or on an empty stomach?
Take it with food. Fat‑soluble vitamins (A, D, E, K) and chelated minerals absorb better with a meal, and food reduces nausea. Splitting the 4 capsules into two meals often feels best.
How long until I notice effects from a multivitamin?
Labs move first: Homocysteine and certain B‑vitamin markers can improve in 4–8 weeks, Vitamin D in 4–12 weeks. Subjective energy changes vary. Recheck Vitamin D, 25-Hydroxy and, if relevant, Homocysteine after 8–12 weeks.
Can I take this with thyroid medication?
Yes, but separate by 4 hours. Minerals like calcium, magnesium, and zinc bind levothyroxine and blunt absorption. Take thyroid first thing with water, then your multivitamin later with a meal.
Does vitamin K in this multivitamin interact with blood thinners?
It interacts with warfarin. Vitamin K changes warfarin’s effect, so avoid this formula unless your prescriber intentionally adjusts your dose. It does not interact the same way with newer anticoagulants.
Will the magnesium here replace a standalone magnesium supplement?
It provides 200 mg of well‑absorbed magnesium, a solid maintenance amount. If you’re using magnesium therapeutically (for constipation, migraines, or sleep), you may still need an additional targeted dose.
Why is my urine bright yellow after taking this?
That’s riboflavin (vitamin B2). It colors urine a vivid yellow when absorbed. It’s normal and not a sign of dehydration or harm.
Can I add iron separately if I need it?
Yes. Many clinicians pair an iron‑free multivitamin with a separate iron dose when Ferritin is low. Take iron away from calcium and magnesium for better absorption, and recheck Ferritin after 8–12 weeks.
How to take it & ingredients
Suggested use: 4 capsules per day with food or as recommended by your health care professional.
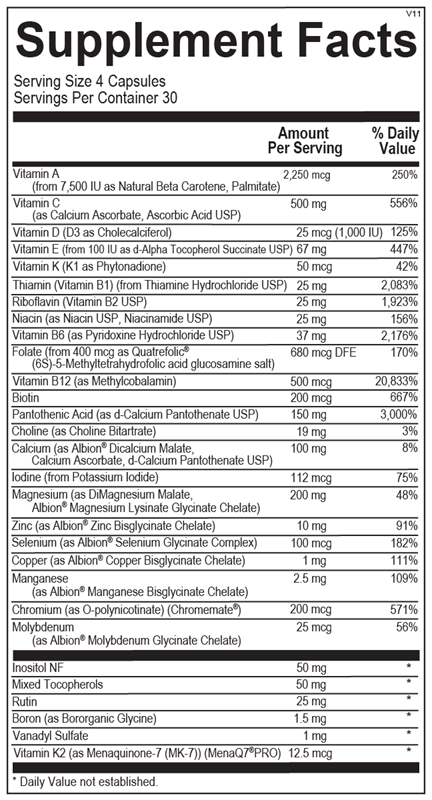
Active ingredients
4 capsules per serving · 30 servings
Vitamin A
From 7,500 IU as Natural Beta Carotene, Palmitate
From 7,500 IU as Natural Beta Carotene, Palmitate
2250 mcg
Vitamin C
As Calcium Ascorbate, Ascorbic Acid USP
As Calcium Ascorbate, Ascorbic Acid USP
500 mg
Vitamin D
D3 as Cholecalciferol
D3 as Cholecalciferol
25 mcg
Vitamin E
From 100 IU as d-Alpha Tocopherol Succinate USP
From 100 IU as d-Alpha Tocopherol Succinate USP
67 mg
Vitamin K
K1 as Phytonadione
K1 as Phytonadione
50 mcg
Thiamin (Vitamin B1)
From Thiamine Hydrochloride USP
From Thiamine Hydrochloride USP
25 mg
Riboflavin (Vitamin B2)
USP
USP
25 mg
Niacin
As Niacin USP, Niacinamide USP
As Niacin USP, Niacinamide USP
25 mg
Vitamin B6
As Pyridoxine Hydrochloride USP
As Pyridoxine Hydrochloride USP
37 mg
Folate
From 400 mcg as Quatrefolic® (6S)-5-Methyltetrahydrofolic acid glucosamine salt
From 400 mcg as Quatrefolic® (6S)-5-Methyltetrahydrofolic acid glucosamine salt
680 mcg DFE
Vitamin B12
As Methylcobalamin
As Methylcobalamin
500 mcg
Biotin
200 mcg
Pantothenic Acid
As d-Calcium Pantothenate USP
As d-Calcium Pantothenate USP
150 mg
Choline
As Choline Bitartrate
As Choline Bitartrate
19 mg
Calcium
As Albion® Dicalcium Malate, Calcium Ascorbate, d-Calcium Pantothenate USP
As Albion® Dicalcium Malate, Calcium Ascorbate, d-Calcium Pantothenate USP
100 mg
Iodine
From Potassium Iodide
From Potassium Iodide
112 mcg
Magnesium
As DiMagnesium Malate, Albion® Magnesium Lysinate Glycinate Chelate
As DiMagnesium Malate, Albion® Magnesium Lysinate Glycinate Chelate
200 mg
Zinc
As Albion® Zinc Bisglycinate Chelate
As Albion® Zinc Bisglycinate Chelate
10 mg
Selenium
As Albion® Selenium Glycinate Complex
As Albion® Selenium Glycinate Complex
100 mcg
Copper
As Albion® Copper Bisglycinate Chelate
As Albion® Copper Bisglycinate Chelate
1 mg
Manganese
As Albion® Manganese Bisglycinate Chelate
As Albion® Manganese Bisglycinate Chelate
2.5 mg
Chromium
As O-polynicotinate (Chromemate®)
As O-polynicotinate (Chromemate®)
200 mcg
Molybdenum
As Albion® Molybdenum Glycinate Chelate
As Albion® Molybdenum Glycinate Chelate
25 mcg
Inositol
NF
NF
50 mg
Mixed Tocopherols
50 mg
Rutin
25 mg
Boron
As Bororganic Glycine
As Bororganic Glycine
1.5 mg
Vanadyl Sulfate
1 mg
Vitamin K2
As Menaquinone-7 (MK-7) (MenaQ7®PRO)
As Menaquinone-7 (MK-7) (MenaQ7®PRO)
12.5 mcg
Other ingredients: Hypromellose (Natural Vegetable Capsules), Magnesium Stearate, Stearic Acid, Silicon Dioxide
Certifications
Benefits
Warnings
Customers also considered

Nature’s Way
Alive! Men’s 50+ Ultra Potency
60 tablets
$29.99extra 20% off with Subscribe & Save

Ortho Molecular Products
Alpha Base® Capsules with Iron
240 capsules
$74.31extra 10% off with Subscribe & Save
Ortho Molecular Products
Alpha Base® Premier Packs
30 packets
$109.50extra 10% off with Subscribe & Save

Thorne
Basic Nutrients 2/Day
60 capsules
$36.00extra 10% off with Subscribe & Save