

Ortho Molecular Products
Alpha Base® Capsules without Iron by Ortho Molecular Products
240 capsules · 60-day supply
Comprehensive Multivitamin Support for Optimal Health and Vitality$74.09
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Alpha Base® Capsules without Iron overview
If you’re looking for a multivitamin without iron, this fits men, post‑menopausal women, and anyone with high Ferritin (the protein that stores iron) or a history of iron intolerance. It’s also a good base if your Vitamin D, 25-Hydroxy is low-normal, B12 or Folate run low, or Homocysteine (a methylation byproduct linked to B-vitamin status) is elevated. Hemochromatosis and frequent blood test–guided phlebotomy patients often use iron-free formulas. Pregnant individuals or those with known iron deficiency should choose a prenatal or a multivitamin with iron instead.
This multivitamin uses methylfolate (Quatrefolic), the bioactive folate form that bypasses common MTHFR enzyme variants, paired with methylcobalamin (active B12) to help normalize Homocysteine within 4 to 12 weeks. It combines vitamin K1 with K2 MK‑7 (longer-acting vitamin K for calcium handling) alongside vitamin D3 for bone and vascular balance. Minerals are chelated (glycinate/malate forms), which are better tolerated and absorbed than oxides. You also get mixed tocopherols (vitamin E family) and 200 mg of chelated magnesium, useful if your dietary magnesium is light.
Take 4 capsules daily with food, ideally split 2 with breakfast and 2 with dinner to improve absorption and reduce nausea. Fat-soluble vitamins (A, D, E, K) absorb better with a meal containing some fat. If you’re tracking labs, recheck Vitamin D, 25-Hydroxy, B12, Folate, and Homocysteine after 8 to 12 weeks. This is a maintenance multivitamin; if your Vitamin D is significantly low, you’ll likely need higher-dose D3 short term under clinician guidance, then step back to this.
Warfarin users should clear this first, as vitamin K can counter its effect; newer blood thinners are not vitamin K–sensitive. Separate from levothyroxine, tetracyclines, and quinolone antibiotics by at least 4 hours because minerals block absorption. The chromium and vanadyl sulfate can enhance insulin action; if you use insulin or sulfonylureas, monitor glucose. The iodine amount suits most adults, but those with active thyroid nodules or thyroid autoimmunity should keep iodine intake consistent and coordinate with their clinician.
Frequently asked questions
Do I need an iron-free multivitamin?
Choose iron-free if you’re male, post‑menopausal, prone to high Ferritin, or get stomach upset from iron. If you’re pregnant, planning pregnancy, or have iron deficiency anemia, you need a multivitamin with iron instead.
Is methylfolate better if I have an MTHFR variant?
Yes. Methylfolate is the active folate form and bypasses the MTHFR enzyme step. It often lowers Homocysteine within 4–12 weeks, especially when paired with methylcobalamin (B12).
How long until a multivitamin changes my labs?
Most changes show in 4–12 weeks. Recheck Vitamin D, 25-Hydroxy after 8–12 weeks, and B12, Folate, and Homocysteine after 4–8 weeks. Magnesium status can take 4–8 weeks to improve.
Can I take this with levothyroxine or antibiotics?
Yes, but separate by at least 4 hours. The calcium, magnesium, and other minerals reduce absorption of levothyroxine, tetracyclines, and quinolone antibiotics if taken together.
Is there enough calcium in this multivitamin for bones?
No. It contains 100 mg, which is not a full calcium dose. It’s designed to pair vitamin D3 and K2 with modest calcium and magnesium. Use separate calcium if your diet is low and your clinician advises it.
Will this multivitamin upset my stomach?
It’s formulated with gentler chelated minerals, but any multivitamin can cause nausea on an empty stomach. Take with meals and split the dose (2 in the morning, 2 in the evening).
Is it safe with blood thinners?
If you take warfarin, talk to your clinician first because vitamin K affects dosing. Direct oral anticoagulants aren’t vitamin K–sensitive, but always confirm with your prescriber.
Can I add extra vitamin D or magnesium?
Often yes. This provides 1,000 IU (25 mcg) of D3 and 200 mg magnesium. If your Vitamin D, 25-Hydroxy is low, higher D3 may be needed short term. Extra magnesium depends on diet and tolerance.
How to take it & ingredients
Suggested use: 4 capsules per day with food or as recommended by your health care professional.
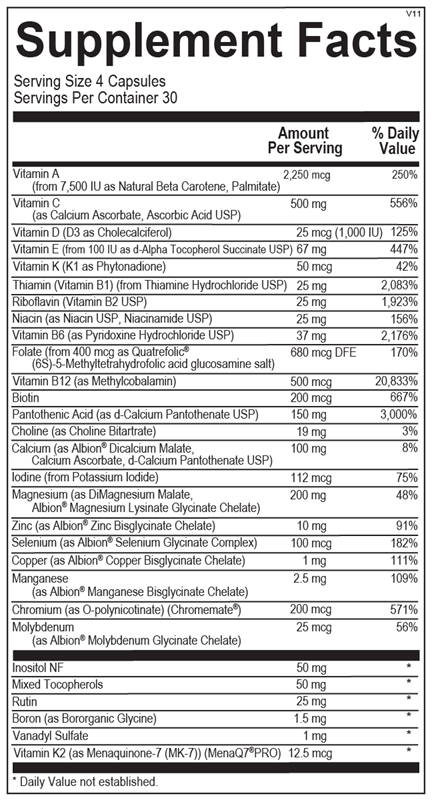
Active ingredients
4 capsules per serving · 60 servings
Vitamin A
From 7,500 IU as Natural Beta Carotene, Palmitate
From 7,500 IU as Natural Beta Carotene, Palmitate
2250 mcg
Vitamin C
As Calcium Ascorbate, Ascorbic Acid USP
As Calcium Ascorbate, Ascorbic Acid USP
500 mg
Vitamin D
D3 as Cholecalciferol
D3 as Cholecalciferol
25 mcg
Vitamin E
From 100 IU as d-Alpha Tocopherol Succinate USP
From 100 IU as d-Alpha Tocopherol Succinate USP
67 mg
Vitamin K
K1 as Phytonadione
K1 as Phytonadione
50 mcg
Thiamin (Vitamin B1)
From Thiamine Hydrochloride USP
From Thiamine Hydrochloride USP
25 mg
Riboflavin (Vitamin B2)
USP
USP
25 mg
Niacin
As Niacin USP, Niacinamide USP
As Niacin USP, Niacinamide USP
25 mg
Vitamin B6
As Pyridoxine Hydrochloride USP
As Pyridoxine Hydrochloride USP
37 mg
Folate
From 400 mcg as Quatrefolic® (6S)-5-Methyltetrahydrofolic acid glucosamine salt
From 400 mcg as Quatrefolic® (6S)-5-Methyltetrahydrofolic acid glucosamine salt
680 mcg DFE
Vitamin B12
As Methylcobalamin
As Methylcobalamin
500 mcg
Biotin
200 mcg
Pantothenic Acid
As d-Calcium Pantothenate USP
As d-Calcium Pantothenate USP
150 mg
Choline
As Choline Bitartrate
As Choline Bitartrate
19 mg
Calcium
As Albion® Dicalcium Malate, Calcium Ascorbate, d-Calcium Pantothenate USP
As Albion® Dicalcium Malate, Calcium Ascorbate, d-Calcium Pantothenate USP
100 mg
Iodine
From Potassium Iodide
From Potassium Iodide
112 mcg
Magnesium
As DiMagnesium Malate, Albion® Magnesium Lysinate Glycinate Chelate
As DiMagnesium Malate, Albion® Magnesium Lysinate Glycinate Chelate
200 mg
Zinc
As Albion® Zinc Bisglycinate Chelate
As Albion® Zinc Bisglycinate Chelate
10 mg
Selenium
As Albion® Selenium Glycinate Complex
As Albion® Selenium Glycinate Complex
100 mcg
Copper
As Albion® Copper Bisglycinate Chelate
As Albion® Copper Bisglycinate Chelate
1 mg
Manganese
As Albion® Manganese Bisglycinate Chelate
As Albion® Manganese Bisglycinate Chelate
2.5 mg
Chromium
As O-polynicotinate (Chromemate®)
As O-polynicotinate (Chromemate®)
200 mcg
Molybdenum
As Albion® Molybdenum Glycinate Chelate
As Albion® Molybdenum Glycinate Chelate
25 mcg
Inositol
NF
NF
50 mg
Mixed Tocopherols
50 mg
Rutin
25 mg
Boron
As Bororganic Glycine
As Bororganic Glycine
1.5 mg
Vanadyl Sulfate
1 mg
Vitamin K2
As Menaquinone-7 (MK-7) (MenaQ7®PRO)
As Menaquinone-7 (MK-7) (MenaQ7®PRO)
12.5 mcg
Other ingredients: Hypromellose (Natural Vegetable Capsules), Magnesium Stearate, Stearic Acid, Silicon Dioxide
Certifications
Benefits
Warnings
Customers also considered

Nature’s Way
Alive! Men’s 50+ Ultra Potency
60 tablets
$29.99extra 20% off with Subscribe & Save

Ortho Molecular Products
Alpha Base® Capsules with Iron
240 capsules
$74.31extra 10% off with Subscribe & Save
Ortho Molecular Products
Alpha Base® Premier Packs
30 packets
$109.50extra 10% off with Subscribe & Save

Thorne
Basic Nutrients 2/Day
60 capsules
$36.00extra 10% off with Subscribe & Save