
Ortho Molecular Products
Cardio MET Pack by Ortho Molecular Products
30 packets · 30-day supply
Comprehensive Metabolic Support for Heart Health and Wellness$153.24
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Corn Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Cardio MET Pack overview
If your Triglycerides run high and your A1c or fasting glucose is creeping up, this combination of omega-3, berberine, bergamot, and alpha-lipoic acid is built for you. Omega-3 for high triglycerides is the anchor here: most responders see a 20–30% drop within 4 to 12 weeks. Berberine modestly lowers fasting glucose and A1c, useful if your A1c is in the higher end of normal. Bergamot targets LDL and non-HDL cholesterol, which tracks with ApoB (the number of atherogenic particles). It’s a practical fit if your Omega-3 Index is low and your hs-CRP (a general inflammation marker) runs elevated.
EPA and DHA (the long-chain omega-3 fats) reduce how much fat your liver exports in VLDL particles (the triglyceride carriers) and can nudge down hs-CRP. Berberine activates AMPK (the cell’s fuel gauge that improves how you use glucose and fat), which helps insulin sensitivity and may reduce PCSK9 (a liver protein that raises LDL). Bergamot polyphenols act at the liver’s cholesterol-making step (the same pathway statins target), improving LDL and non-HDL. Alpha-lipoic acid regenerates antioxidants like glutathione and improves insulin sensitivity, especially when glucose is high.
Take one daily packet with a meal that contains some fat; omega-3 absorbs better with food and you’ll reduce fishy burps. The 1,900 mg total omega-3 as triglycerides is a clinically useful dose for triglycerides. Berberine at 500 mg once daily is an entry dose; many protocols use 500 mg two to three times daily with meals for glucose control, so your clinician may add a separate berberine capsule if labs warrant. Expect triglyceride changes in 4–12 weeks and A1c changes over 8–12 weeks.
If you use insulin or sulfonylureas, berberine and alpha-lipoic acid can lower glucose further; monitor and coordinate dose changes. Berberine interacts with cyclosporine, tacrolimus, and many drugs moved by CYP3A4/P-glycoprotein. Bergamot plus a statin is additive for LDL; report new muscle pain. High-dose omega-3 has a small bleeding signal; use caution with warfarin and other blood thinners. Pregnancy and breastfeeding: avoid berberine. Significant liver or kidney disease: use only with clinician oversight.
Frequently asked questions
How long until triglycerides drop with omega-3?
Most people who respond see triglycerides fall within 4 to 12 weeks. Take omega-3 with food daily and recheck a lipid panel after about 8 to 12 weeks to confirm.
Is 500 mg berberine enough for blood sugar?
It’s a conservative starting dose. Many trials use 500 mg two to three times daily with meals. If fasting glucose or A1c stay high, your clinician may increase or split dosing.
Does fish oil thin your blood?
Omega-3 can modestly increase bleeding time, but the effect is small. If you’re on warfarin or other blood thinners, discuss dosing and monitoring with your clinician.
Can I take this with a statin or ezetimibe?
Often, yes. Omega-3 pairs well, and bergamot may be additive for LDL. Watch for new muscle symptoms on statins and check liver enzymes as your clinician advises.
What labs should I track while using this pack?
Check a lipid panel (Triglycerides, LDL, non-HDL), ApoB if available, Omega-3 Index, fasting glucose, A1c, and hs-CRP. Reassess in 8–12 weeks to gauge response.
Does berberine cause stomach issues?
It can cause constipation, cramping, or loose stools, especially when starting. Taking it with meals and adequate hydration usually helps. Reduce or split the dose if needed.
Is bergamot the same as grapefruit for drug interactions?
No, bergamot isn’t grapefruit, but it can still interact at the liver’s enzyme systems. If you’re on narrow-therapeutic-index drugs, clear it with your prescriber.
Can I take alpha-lipoic acid at night?
You can, but taking the pack with a meal is simpler and may reduce nausea. Alpha-lipoic acid can lower glucose, so be consistent with timing relative to meals and meds.
How to take it & ingredients
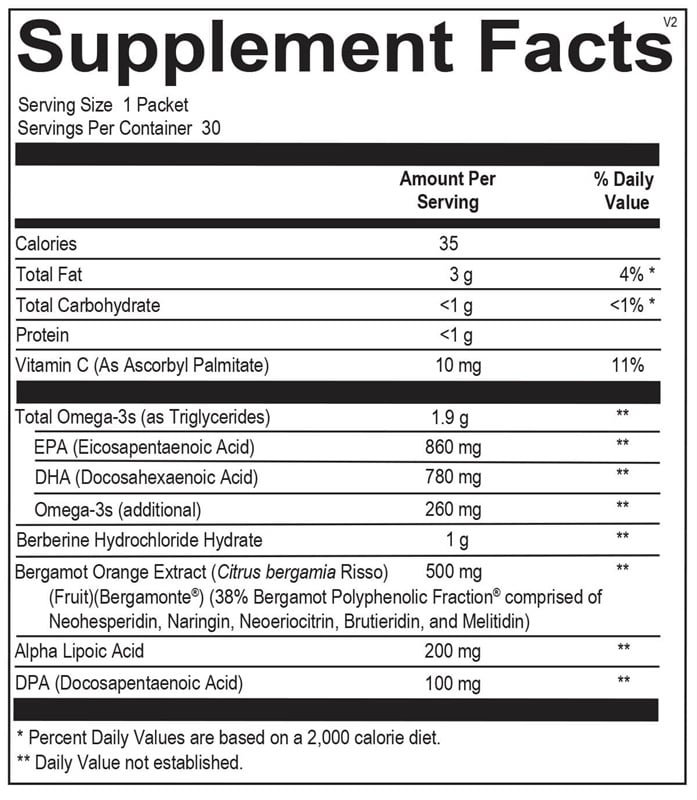
Suggested use: 1 packet per day or as recommended by your health care professional.
Active ingredients
1 packet per serving · 30 servings
▼
Total Omega-3s
As Triglycerides
As Triglycerides
1900 mg
EPA (Eicosapentaenoic Acid)
860 mg
DHA (Docosahexaenoic Acid)
780 mg
DPA (Docosapentaenoic Acid)
100 mg
Omega-3s (additional)
260 mg
Berberine Hydrochloride Hydrate
500 mg
Bergamot Orange Extract
Citrus bergamia Risso (Fruit) (Bergamonte®) (38% Bergamot Polyphenolic Fraction® comprised of Neohesperidin, Naringin, Neoeriocitrin, Brutieridin, and Melitidin)
Citrus bergamia Risso (Fruit) (Bergamonte®) (38% Bergamot Polyphenolic Fraction® comprised of Neohesperidin, Naringin, Neoeriocitrin, Brutieridin, and Melitidin)
200 mg
Alpha Lipoic Acid
1000 mg
Vitamin C
As Ascorbyl Palmitate
As Ascorbyl Palmitate
10 mg
Other ingredients: Fish Oil (anchovy, jack mackerel, mackerel, sardine) (Highly Refined and Concentrated Omega-3), Gelatin, Microcrystalline Cellulose, Hypromellose (Natural Vegetable Capsules), Glycerin, Magnesium Stearate, Water (Purified), Natural Flavors, Silicon Dioxide, Stearic Acid, Natural Tocopherols, Rosemary Extract (Leaf), Sunflower Oil
Certifications
Benefits
Warnings
Customers also considered

Calocurb
Calocurb Amarasate Appetite Control
90 capsules
$89.99extra 20% off with Subscribe & Save

Ortho Molecular Products
Core Restore 14-Day Kit (Chocolate)
14 day kits
$239.76extra 10% off with Subscribe & Save

Ortho Molecular Products
Core Restore 14-Day Kit (French Vanilla)
14 day kits
$239.76extra 10% off with Subscribe & Save

Ortho Molecular Products
Core Restore 7-Day Kit (Chocolate)
7 day kits
$146.69extra 10% off with Subscribe & Save