

Ortho Molecular Products
Liquid Vitamin D3 with K2 by Ortho Molecular Products
30 milliliters · 1200-day supply
Essential Vitamins for Bone Health and Cardiovascular Support$52.00
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Corn Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Liquid Vitamin D3 with K2 overview
If your Vitamin D, 25-Hydroxy is in the lower part of the normal range and you want a simple maintenance plan, vitamin D3 with K2 drops are a clean fit. They suit adults with little sun, darker skin, consistent sunscreen use, or northern latitude winters. The 1,000 IU D3 here is maintenance-level; if your level is meaningfully low or you have higher body weight, you’ll likely need a larger repletion dose short‑term, then step down. Vegans, dairy-avoiders, and post-menopausal women often find the K2 addon useful for bone strategy.
Cholecalciferol (vitamin D3) is the form your skin makes from sunlight. Your liver and kidneys convert it to the active hormone that raises calcium absorption and helps keep parathyroid hormone (PTH, the signal that pulls calcium from bone) in check. Vitamin K2 as MK-7 activates osteocalcin (a bone-building protein that locks calcium into bone) and matrix Gla-protein, or MGP (a protein that helps keep calcium out of artery walls). Evidence for artery calcification protection is promising but mixed; for bones, D3 plus K2 is a rational pair when calcium intake is adequate.
One drop daily delivers 1,000 IU D3 plus 10 mcg K2 (MK-7). Take it with a meal that contains fat for best absorption, directly on the tongue or mixed in a beverage. Re-test Vitamin D, 25-Hydroxy after 8–12 weeks to confirm you’re on target. Most K2 MK-7 trials use 90–180 mcg per day, so the K2 here is a light, maintenance add-on rather than a high-dose K2 strategy.
Skip K2 if you take warfarin (Coumadin), since vitamin K interferes with how that drug thins blood. Direct oral anticoagulants like apixaban or rivaroxaban are not affected the same way, but ask your clinician. If you have a history of high calcium, recurrent kidney stones, sarcoidosis, or hyperparathyroidism, use D3 only with medical guidance. Thiazide diuretics can raise calcium; combining with high-dose D3 needs monitoring. In pregnancy, maintenance D3 is routine, but clear K2 use with your OB.
Frequently asked questions
Is vitamin D3 with K2 better than vitamin D alone?
For bone strategy, pairing D3 with K2 is sensible: D3 raises calcium absorption, K2 activates proteins that direct calcium into bone. For cardiovascular outcomes, human trials are mixed. If your Vitamin D, 25-Hydroxy is low, prioritize raising D3 first, then consider adding or adjusting K2.
How long does vitamin D3 take to raise my lab levels?
Most people see meaningful changes in Vitamin D, 25-Hydroxy within 8–12 weeks at a steady daily dose. The 1,000 IU here is maintenance. If you’re starting from a low level, clinicians often use higher short-term dosing, then step back to maintenance and re-test.
Is 1,000 IU of vitamin D3 enough for me?
It’s a maintenance dose for many adults with levels in the low-normal range. If your level is significantly low, or you have higher body weight, limited sun, or malabsorption, you’ll likely need more initially under clinician guidance, then drop to 1,000 IU and re-check your labs.
Can I take vitamin D3 with K2 if I’m on blood thinners?
Avoid K2 if you take warfarin (Coumadin), because vitamin K counteracts its effect. If you’re on apixaban, rivaroxaban, or similar, that interaction doesn’t apply, but still review supplements with your prescriber.
Do I need to take these drops with food?
Yes, take with a meal that has some fat to improve absorption of both D3 and K2. Timing during the day isn’t critical. Pick a consistent time that helps you remember, and stick with it.
Should I take calcium with vitamin D3 and K2?
Only if your diet is low in calcium. D3 and K2 help direct calcium, but they don’t replace intake. Aim to meet most calcium from food; add a supplement only if you can’t meet needs and after reviewing your kidney stone risk.
Which labs should I monitor while taking vitamin D3 with K2?
Check Vitamin D, 25-Hydroxy after 8–12 weeks. If you have a history of high calcium or are on thiazide diuretics, your clinician may also follow serum calcium and PTH (parathyroid hormone, which regulates bone turnover).
How to take it & ingredients
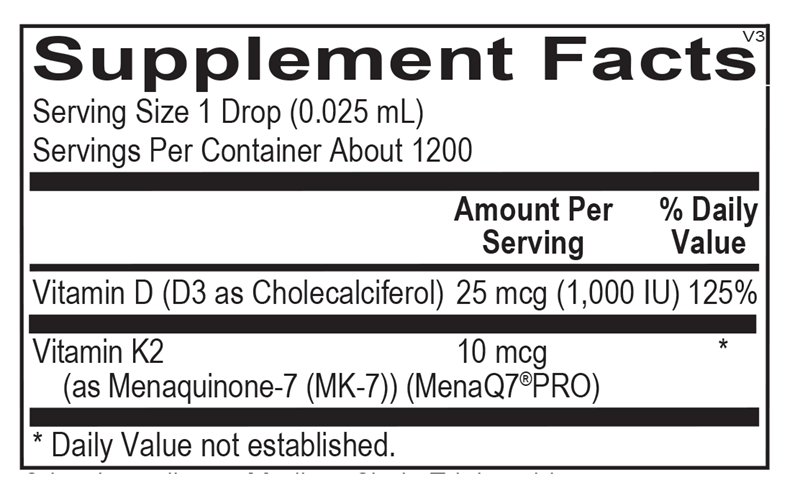
Suggested use: Take 1 drop (0.025 mL) per day or as recommended by your health care professional. Can be taken directly on the tongue and swallowed or mixed with the beverage of your choice.
Active ingredients
1 drop = 0.025 mL per serving · 1200 servings
Vitamin D
D3 as Cholecalciferol
D3 as Cholecalciferol
25 mcg, 1000 IU
Vitamin K2
As Menaquinone-7 (MK-7) (MenaQ7® PRO)
As Menaquinone-7 (MK-7) (MenaQ7® PRO)
10 mcg
Other ingredients: Medium Chain Triglycerides
Certifications
Benefits
Warnings
Customers also considered

Life Extension
Bone Restore Calcium Supplement with Vitamin K2
120 capsules
$24.99extra 20% off with Subscribe & Save

Ortho Molecular Products
K-FORCE
60 capsules
$60.33extra 10% off with Subscribe & Save

Ortho Molecular Products
K-FORCE MAX
30 capsules
$44.79extra 10% off with Subscribe & Save

NBI
Osteo-K Minis
120 capsules
$65.99extra 20% off with Subscribe & Save