

NBI
Osteo-K Minis by NBI
120 capsules · 60-day supply
Essential Support for Bone Health and Calcium Absorption$65.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Dairy Free
NBI Osteo-K Minis overview
If a DXA scan shows low bone density, or you’re post‑menopausal or on long-term steroids, vitamin K2 MK-4 with calcium citrate and vitamin D3 is a targeted stack. It’s useful when your Vitamin D, 25-Hydroxy is in the lower end of normal and you want a maintenance dose, not a repletion plan. Dairy-light eaters and adults with high bone turnover markers (P1NP and CTX, the lab signals of bone remodeling) are common fits.
MK-4 (a form of vitamin K2) activates osteocalcin and matrix Gla protein, the proteins that guide calcium into bone and keep it out of arteries. Clinical trials in Japan used multi‑milligram MK-4 to maintain bone density and reduce vertebral fractures. Vitamin D3 raises calcium absorption and keeps parathyroid hormone (the signal that pulls calcium from bone) in check. Calcium citrate supplies absorbable calcium and is gentler for people with sensitive stomachs.
Take 2 capsules twice daily with meals as directed; fat in a meal improves absorption of vitamin K2 MK-4 and vitamin D3, and splitting calcium improves uptake. The 25 mcg D3 is a maintenance dose; if your Vitamin D, 25-Hydroxy is low, repletion usually needs higher doses short term. The 200 mg calcium citrate here is supplemental, so count your diet to reach an appropriate daily total.
Do not use vitamin K2 MK-4 with warfarin or other vitamin K–antagonist blood thinners; it opposes their effect. Separate calcium from levothyroxine by 4 hours, and from tetracyclines or fluoroquinolones by at least 2–6 hours to avoid blocking absorption. Take calcium away from morning bisphosphonates. If you have high calcium, primary hyperparathyroidism, sarcoidosis, or significant kidney disease, talk with your clinician first.
Frequently asked questions
What’s the difference between MK-4 and MK-7 vitamin K2?
MK-4 is the short-chain form used in Japanese osteoporosis trials at multi‑milligram doses. MK-7 has a longer half-life and is often used at microgram doses. For bone density, high-dose MK-4 has the most fracture data; MK-7 has solid carboxylation data but fewer fracture trials.
How long does vitamin K2 MK-4 take to affect bones?
Bone turnover markers like P1NP and CTX can shift within 4–12 weeks. Meaningful changes in bone density on DXA are typically assessed over 6–12 months. Stay consistent and recheck labs and scans on that timeline with your clinician.
Can I take this with warfarin?
No. Vitamin K2 MK-4 counteracts warfarin and other vitamin K–antagonist anticoagulants. If you need vitamin K while anticoagulated, that requires clinician-managed dosing and INR monitoring. Do not start on your own.
Do I need extra vitamin D with this?
If your Vitamin D, 25-Hydroxy is low, you’ll likely need a higher short-term D3 dose than the 25 mcg here, then step down to maintenance. Get your level checked and follow a repletion plan from your clinician.
When should I take the calcium in this?
Take with meals and split doses, which improves absorption and reduces stomach upset. Separate by 4 hours from levothyroxine, and by at least 2–6 hours from tetracyclines or fluoroquinolone antibiotics to avoid blocking their absorption.
Is vitamin K2 MK-4 safe in pregnancy?
High-dose MK-4 hasn’t been established as safe in pregnancy or breastfeeding. Stick to prenatal-vitamin levels of vitamin K unless your OB advises otherwise. Calcium and vitamin D needs may rise; discuss targeted dosing with your clinician.
Can I use this with a bisphosphonate or denosumab?
Often yes, as an adjunct. Take bisphosphonates first thing with water and no calcium; add calcium and vitamin D3 later with meals. Bring all supplements to your bone clinic so dosing and timing fit your prescription.
What labs should I monitor on this?
Track Vitamin D, 25-Hydroxy for dose adequacy, serum calcium to avoid excess, and bone turnover markers (P1NP and CTX) to gauge response. Your long-term outcome is best assessed by DXA at 1–2 year intervals.
How to take it & ingredients
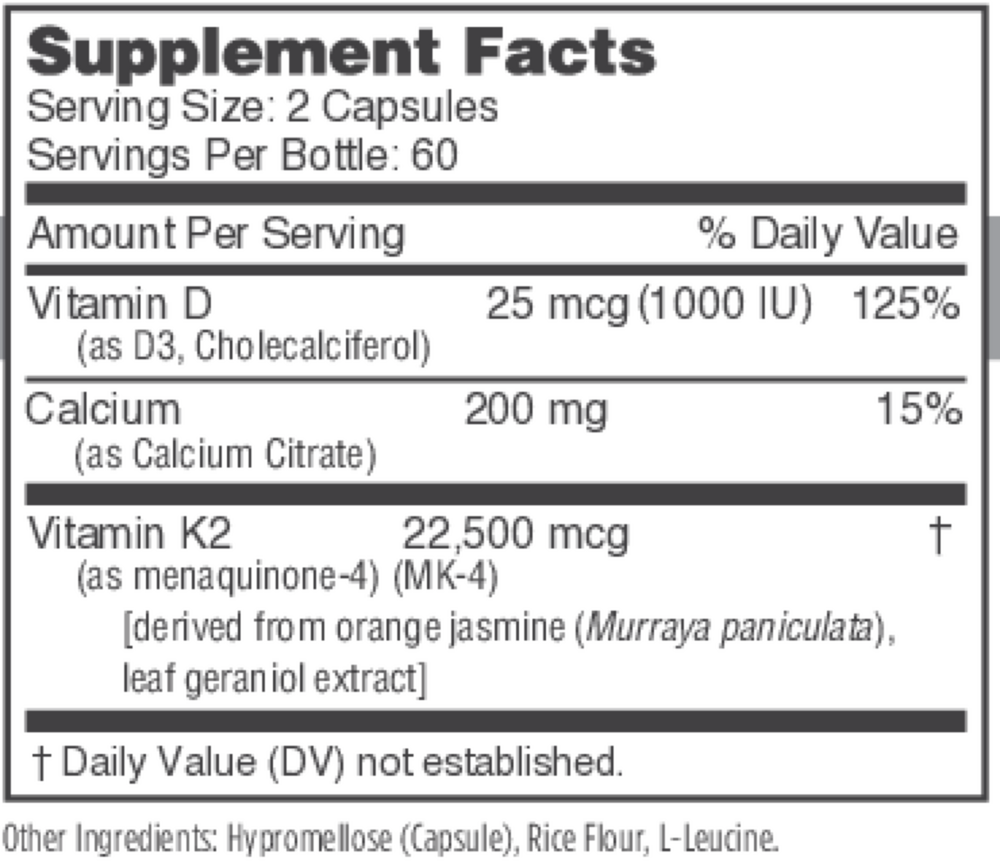
Suggested use: Take 2 capsules twice a day with meals or as directed by a healthcare professional.
Active ingredients
2 capsules per serving · 60 servings
Vitamin D
Cholecalciferol (D3)
Cholecalciferol (D3)
25 mcg, 1000 IU
Vitamin K
Menaquinone 4 (MK-4)
Menaquinone 4 (MK-4)
22500 mcg
Calcium
Calcium Citrate
Calcium Citrate
200 mg
Other ingredients: Hypromellose (vegetarian capsule), Rice flour, L-leucine
Certifications
Benefits
Warnings
Customers also considered

Ortho Molecular Products
K-FORCE
60 capsules
$60.33extra 10% off with Subscribe & Save

Ortho Molecular Products
K-FORCE MAX
30 capsules
$44.79extra 10% off with Subscribe & Save

Ortho Molecular Products
Liquid Vitamin D3 with K2
30 milliliters
$52.00extra 10% off with Subscribe & Save

Natura Health Products
VITAMIN D-A-K
60 capsules
$24.99extra 20% off with Subscribe & Save