

Ortho Molecular Products
K-FORCE by Ortho Molecular Products
60 capsules · 60-day supply
Essential Vitamins for Bone Health and Cardiovascular Support$60.33
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products K-FORCE overview
If your Vitamin D, 25-Hydroxy is low or in the lower-normal range, a daily vitamin D3 and K2 capsule like this fits as a repletion-leaning dose. It’s practical for darker-skinned adults, indoor or northern-latitude lifestyles, and post-menopausal women focused on bone density. It also suits people with low dietary vitamin K2 intake (few fermented foods). If your level is already robust, this is more than a maintenance dose, so retest and adjust.
Vitamin D3 raises calcium absorption from the gut and helps dial down parathyroid hormone (the signal that pulls calcium from bone). Vitamin K2 as MK-7 activates osteocalcin (the protein that locks calcium into bone) and matrix Gla protein (the protein that helps keep calcium out of artery walls). MK-7 has a longer half-life than K1 or MK-4, so it stays active through the day. Expect Vitamin D, 25-Hydroxy to rise within 4–8 weeks; bone turnover shifts take months.
Take 1 capsule daily with a meal that contains fat for absorption. 5,000 IU of vitamin D3 is often used short term if your level is low, then many people step down once replete. Recheck Vitamin D, 25-Hydroxy after 8–12 weeks, and consider Calcium and parathyroid hormone on the same draw. Adequate dietary calcium and magnesium matter; low magnesium can blunt vitamin D response.
Skip K2 if you use warfarin or similar vitamin K–blocking blood thinners; dose stability of these drugs depends on consistent vitamin K, so involve your prescriber. Thiazide diuretics (blood pressure pills that reduce calcium loss) plus high-dose D3 can raise calcium. Orlistat (fat-blocking weight-loss drug) and bile acid sequestrants like cholestyramine (cholesterol binders) reduce absorption of fat-soluble vitamins; separate by several hours.
Use clinician guidance if you have a history of high calcium, recurrent calcium kidney stones, hyperparathyroidism, sarcoidosis or other granulomatous disease (these can overshoot active vitamin D), severe kidney disease, or you’re pregnant and considering more than a maintenance dose. If your Vitamin D, 25-Hydroxy is already high, lower-dose vitamin D3 without extra K2 is usually more appropriate.
Frequently asked questions
Do I need to take vitamin D3 and K2 together?
They target different steps. D3 raises calcium absorption; K2 activates proteins that put calcium into bone and keep it out of arteries. Pairing them is reasonable when raising D with a meaningful dose, especially if your diet is low in K2.
How long does it take to raise my vitamin D level?
Most people see Vitamin D, 25-Hydroxy rise within 4–8 weeks on a 5,000 IU daily dose. Retest at 8–12 weeks and adjust to a maintenance dose if you’ve reached your target range.
Is 5,000 IU of vitamin D3 too much to take every day?
It’s a common short-term dose when your level is low, but it’s higher than typical maintenance for many adults. The right dose depends on your Vitamin D, 25-Hydroxy, body weight, sun exposure, and goals. Retesting guides the step-down.
Should I take vitamin D3 K2 with food or on an empty stomach?
Take it with a meal that contains fat. D3 and K2 are fat-soluble and absorb better with dietary fat. Morning or evening is fine—consistency matters more than timing.
Is vitamin K2 safe with blood thinners like warfarin?
No. Warfarin and similar drugs work by blocking vitamin K recycling. K2 can change your INR. Do not use K2 unless your prescriber adjusts your therapy and monitors levels. Direct oral anticoagulants are different; still ask your clinician.
What labs should I monitor while taking D3 and K2?
Track Vitamin D, 25-Hydroxy after 8–12 weeks. Consider Calcium and parathyroid hormone on the same draw. If you have a history of stones or high calcium, monitoring is especially important.
What are signs I’m getting too much vitamin D?
High calcium can cause nausea, constipation, thirst, frequent urination, or confusion. If these occur, stop the supplement and get Calcium and Vitamin D, 25-Hydroxy checked promptly.
Is the vitamin D3 in this product vegan?
Most D3 is sourced from lanolin (sheep’s wool). If you need vegan D3 (from lichen), check the label or contact the manufacturer. Vitamin K2 MK-7 is typically produced by fermentation and is vegan.
How to take it & ingredients
Suggested use: 1 capsule per day or as recommended by your health care professional.
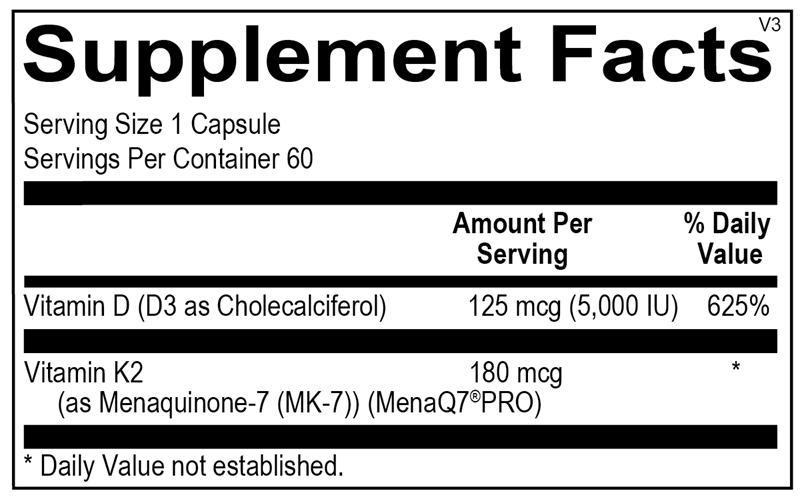
Active ingredients
1 capsule per serving · 60 servings
Vitamin D3
Cholecalciferol
Cholecalciferol
5000 IU
Vitamin K2
As MK-7 (MenaQ7 PRO)
As MK-7 (MenaQ7 PRO)
180 mcg
Other ingredients: Microcrystalline Cellulose, Hypromellose (Natural Vegetable Capsule), Turmeric (color), Magnesium Stearate, Silicon Dioxide, Stearic Acid
Certifications
Benefits
Warnings
Customers also considered

Ortho Molecular Products
K-FORCE MAX
30 capsules
$44.79extra 10% off with Subscribe & Save

Ortho Molecular Products
Liquid Vitamin D3 with K2
30 milliliters
$52.00extra 10% off with Subscribe & Save

NBI
Osteo-K Minis
120 capsules
$65.99extra 20% off with Subscribe & Save

Natura Health Products
VITAMIN D-A-K
60 capsules
$24.99extra 20% off with Subscribe & Save