

Ortho Molecular Products
Ortho Biotic 100 by Ortho Molecular Products
60 capsules · 60-day supply
Powerful Probiotic Support for Digestive and Immune Health$152.68
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Vegetarian·Gluten Free·Soy Free·Corn Free·Yeast Free·
Ortho Molecular Products Ortho Biotic 100 overview
Post‑antibiotic gut recovery is the most common reason to reach for a 100 billion CFU probiotic. If you’ve just finished antibiotics, have frequent travel‑related diarrhea, or your stool test shows low Lactobacillus/Bifidobacterium on a Comprehensive Stool Analysis, this higher dose makes sense. It’s also reasonable if bloating and loose stools persist despite diet changes. For day‑to‑day maintenance when you feel well, a lower‑dose probiotic is usually enough.
Lactobacillus and Bifidobacterium strains make lactic acid, which gently lowers gut pH and makes it harder for problem microbes to overgrow. They also compete for space and nutrients, reinforce the mucus barrier that lines the intestine, and produce short‑chain fatty acids like acetate that feed colon cells. Clinically, this is why probiotics lower the risk of antibiotic‑associated diarrhea and can reduce bloating in some irritable bowel patterns. Some users also see small drops in hs-CRP (a blood marker of inflammation) when the gut calms down.
One capsule daily is the manufacturer’s guidance. Take with a small meal to buffer stomach acid if you’re sensitive; otherwise any consistent time works. If you’re on antibiotics, separate the probiotic by at least 2–3 hours and continue for 1–2 weeks after the last dose. Expect stool consistency and bloating to shift within 1 to 2 weeks, with steadier changes by 4 weeks. If you’re very reactive, start with every other day for the first week.
Antibiotics can kill the strains in a probiotic, so timing matters; separation preserves more live organisms. Antifungal drugs don’t directly target bacteria but often come with disrupted gut flora, where a probiotic still helps. Check the label for storage; many high‑CFU formulas retain potency longer when refrigerated. If you track labs, improvements often parallel calmer fecal calprotectin (a stool marker of gut inflammation).
Avoid high‑dose probiotics if you are severely immunocompromised (such as active chemotherapy with low neutrophils), have a central venous catheter, or are critically ill. There have been rare bloodstream infections linked to probiotics in these settings. History of severe acute pancreatitis is another reason to avoid. Pregnancy is generally considered low risk with standard probiotics, but discuss dosing with your clinician.
Frequently asked questions
Do I really need a 100 billion CFU probiotic?
Use a high‑dose probiotic when you’re recovering from antibiotics or have persistent loose stools and bloating. For routine maintenance when you feel well, lower CFU counts usually suffice and are more cost‑effective.
How long does a probiotic take to work?
Most people notice changes in stool form and gas within 1–2 weeks, with steadier improvements by 4 weeks. If nothing changes by 4–6 weeks, reassess strain choice, dose, or look for diet and medication contributors.
Should I take probiotics with antibiotics?
Yes, but separate them by 2–3 hours to reduce kill‑off. Continue the probiotic for 1–2 weeks after finishing antibiotics to lower the risk of antibiotic‑associated diarrhea.
Can probiotics cause gas or bloating at first?
They can. Temporary gas, bloating, or a shift in stool frequency is common in the first few days. Starting every other day or with food often smooths the transition. Symptoms usually settle within a week.
Do I need to refrigerate this probiotic?
Refrigeration often preserves potency in high‑CFU products, but follow the label. Many are shelf‑stable for shipping yet keep their count longer when stored cold at home.
Is a higher CFU probiotic always better?
No. Match dose to the job: higher CFU for recovery or stubborn symptoms, standard CFU for daily upkeep. Strain selection and consistency of use matter as much as the number.
Is a probiotic safe during pregnancy?
Typical Lactobacillus and Bifidobacterium probiotics are considered low risk in pregnancy, but discuss dosing with your obstetric clinician. Start low if you’re sensitive to GI changes.
Can I open the capsule and mix it with food?
Usually yes. Sprinkling contents onto cool, soft food or in water is fine. Avoid hot liquids, which can damage live organisms. If you have severe sensitivities, keep the capsule intact.
How to take it & ingredients
Suggested use: Take 1 capsule per day or as recommended by your health care professional.
Active ingredients
1 capsule per serving · 60 servings
▼
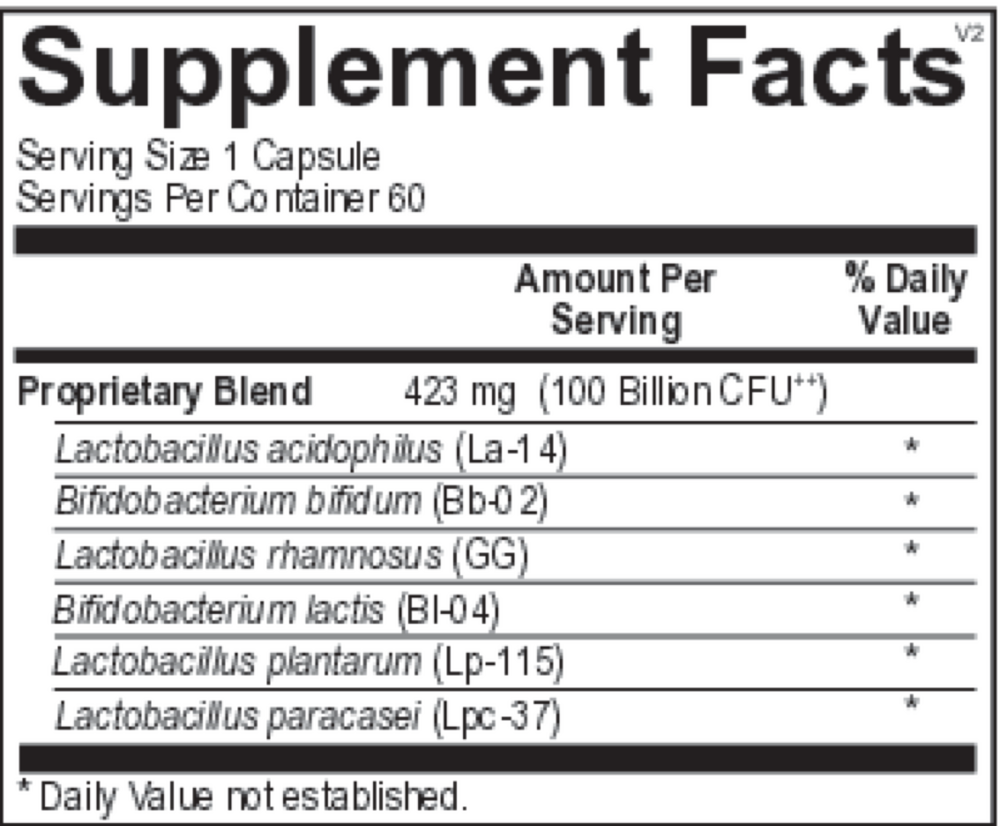
Proprietary Blend
100 billion CFU, 423 mg
Lactobacillus acidophilus (La-14)
-
Bifidobacterium bifidum (Bb-02)
-
Lactobacillus plantarum (Lp-115)
-
Bifidobacterium lactis (Bl-04)
-
Lactobacillus rhamnosus (Lr-32)
-
Lactobacillus paracasei (Lpc-37)
-
Other ingredients: Natural Vegetable Capsules, Microcrystalline Cellulose, Silicon Dioxide, Magnesium Stearate
Certifications
Benefits
Warnings
Customers also considered

Thorne
Bacillus Coagulans
60 capsules
$33.00extra 10% off with Subscribe & Save

Thorne
Complete Biotic
30 packets
$46.00extra 10% off with Subscribe & Save
Dr. Mercola
Complete Probiotics 70 Billion CFU
30 capsules
$46.99extra 19% off with Subscribe & Save
Garden of Life
Dr. Formulated Probiotics Mens Daily Care
30 capsules
$45.99extra 20% off with Subscribe & Save