
Ortho Molecular Products
Prenatal Complete with DHA by Ortho Molecular Products
6 packs
Comprehensive Prenatal Support with Essential Nutrients and DHA for Expecting Mothers$89.08
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Wheat Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Prenatal Complete with DHA overview
Planning pregnancy in the next few months and not eating much seafood is the most common reason to choose prenatal vitamins with DHA. The 580 mg DHA here is a meaningful dose for fetal brain and retina development, and the 30 mg gentle iron fits people whose Ferritin (iron storage) runs low. It also suits those who prefer methylfolate over folic acid, or whose Omega-3 Index or Vitamin D, 25-Hydroxy is in the lower range. If your Ferritin is high, you may not need an iron-containing prenatal.
This formula uses Quatrefolic methylfolate, the active folate that does not require conversion, helpful for those with reduced MTHFR enzyme activity. Methylcobalamin (vitamin B12) and choline support methylation, the cell process that builds DNA and neural tissue. DHA and EPA are long-chain omega-3 fats; DHA is preferentially used to build the fetal brain and eyes. Iron bisglycinate is a chelated form many patients tolerate with less constipation. Iodine supports thyroid hormone production for normal fetal growth, and vitamin D3 aids calcium absorption for bone development.
Take 3 capsules and 1 softgel daily with food. Many feel best splitting the dose with breakfast and dinner to reduce nausea or fishy burps. Start at least 1 to 3 months before conception and continue through breastfeeding. Separate the iron-containing capsules by at least 2 hours from coffee or tea and from calcium-heavy meals, which reduce absorption. If you use levothyroxine, keep iron and calcium 4 hours away to avoid interference.
Skip iron-containing prenatals if you have hemochromatosis or consistently high Ferritin unless your clinician advises otherwise. Avoid if you have a fish or fish-oil allergy, since the DHA softgel is marine-derived. Do not stack with separate retinol vitamin A or cod liver oil; this prenatal already covers vitamin A as beta carotene. If your Omega-3 Index is very low, a stand-alone fish oil may be needed in addition to a prenatal with DHA.
Frequently asked questions
When should I start taking a prenatal with DHA?
Start 1 to 3 months before trying to conceive. Folate and iron status, Vitamin D, 25-Hydroxy, and the Omega-3 Index improve over weeks, not days, and early pregnancy is when demands rise fastest.
Can I take this with my thyroid medication?
Yes, but separate by 4 hours. Iron and calcium can bind levothyroxine and reduce absorption. Take the thyroid pill on an empty stomach, then the prenatal later with food.
Do I still need extra folic acid if this has methylfolate?
Usually no. This provides 1,000 mcg of methylfolate, the active form. Adding more folic acid rarely adds benefit and can complicate lab interpretation unless your clinician directs it.
Will the DHA cause fishy burps?
Occasionally. Taking the softgel with a full meal, keeping it cold until use, and splitting doses reduce aftertaste. If it persists, take it at dinner or before bed.
Is this prenatal vegan?
No. The DHA softgel is marine-derived. If you need a vegan option, look for an algal DHA prenatal and match the DHA amount as closely as possible.
Can I take extra iron with this?
Only if your clinician recommends it. This already includes 30 mg of iron as bisglycinate. Extra iron can raise Ferritin excessively or worsen constipation without clear benefit.
How long to see changes in omega-3 levels?
The Omega-3 Index typically rises within 4 to 12 weeks at consistent daily intake. Retesting after 8 to 12 weeks shows whether your DHA intake is adequate.
Is iodine safe if I have thyroid issues?
Most pregnant patients need iodine, but dosing should be individualized. This contains 150 mcg. If you have thyroid disease or take antithyroid drugs, confirm with your endocrinologist first.
How to take it & ingredients
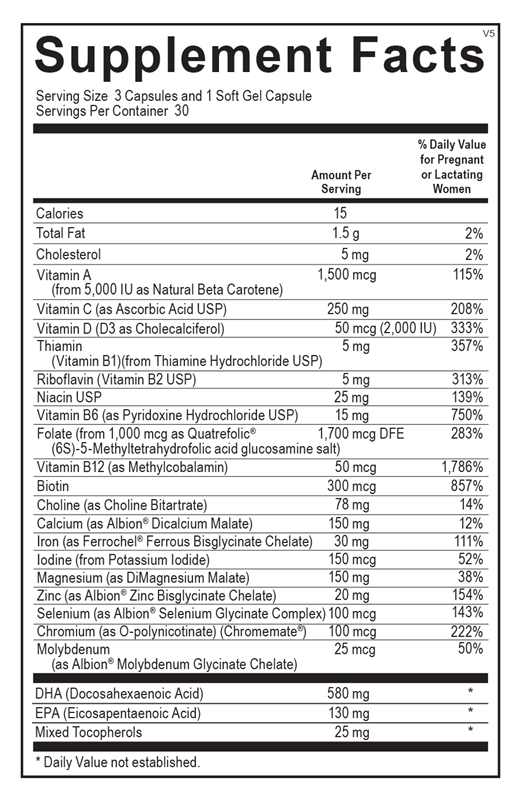
Suggested use: 3 capsules and 1 soft gel per day or as recommended by your health care professional.
Active ingredients
3 capsules per serving
Vitamin A
From Natural Beta Carotene (5,000 IU)
From Natural Beta Carotene (5,000 IU)
1500 mcg
Vitamin C
As Ascorbic Acid USP
As Ascorbic Acid USP
250 mg
Vitamin D
D3 as Cholecalciferol
D3 as Cholecalciferol
50 mcg, 2000 IU
Thiamin (Vitamin B1)
From Thiamine Hydrochloride USP
From Thiamine Hydrochloride USP
5 mg
Riboflavin (Vitamin B2)
USP
USP
5 mg
Niacin
USP
USP
25 mg
Vitamin B6
As Pyridoxine Hydrochloride USP
As Pyridoxine Hydrochloride USP
15 mg
Folate
From Quatrefolic® (6S)-5-Methyltetrahydrofolic acid glucosamine salt (1,000 mcg)
From Quatrefolic® (6S)-5-Methyltetrahydrofolic acid glucosamine salt (1,000 mcg)
1700 mcg DFE
Vitamin B12
As Methylcobalamin
As Methylcobalamin
50 mcg
Biotin
300 mcg
Choline
As Choline Bitartrate
As Choline Bitartrate
78 mg
Calcium
As Albion® Dicalcium Malate
As Albion® Dicalcium Malate
150 mg
Iron
As Ferrochel® Ferrous Bisglycinate Chelate
As Ferrochel® Ferrous Bisglycinate Chelate
30 mg
Iodine
From Potassium Iodide
From Potassium Iodide
150 mcg
Magnesium
As DiMagnesium Malate
As DiMagnesium Malate
150 mg
Zinc
As Albion® Zinc Bisglycinate Chelate
As Albion® Zinc Bisglycinate Chelate
20 mg
Selenium
As Albion® Selenium Glycinate Complex
As Albion® Selenium Glycinate Complex
100 mcg
Chromium
As O-polynicotinate (Chromemate®)
As O-polynicotinate (Chromemate®)
100 mcg
Molybdenum
As Albion® Molybdenum Glycinate Chelate
As Albion® Molybdenum Glycinate Chelate
25 mcg
DHA (Docosahexaenoic Acid)
580 mg
EPA (Eicosapentaenoic Acid)
130 mg
Mixed Tocopherols
20 mg
Other ingredients: Fish Oil (anchovy, jack mackerel, mackerel, sardine), Gelatin, Hypromellose (Natural Vegetable Capsules), Glycerin, Microcrystalline Cellulose, Stearic Acid, Purified Water, Natural Flavors, Magnesium Stearate, Silicon Dioxide, Rosemary Extract (Leaf), Ascorbyl Palmitate
Certifications
Benefits
Warnings
Customers also considered

MegaFood
Baby & Me 2
60 tablets
$47.99extra 21% off with Subscribe & Save

Thorne
Basic Prenatal
90 capsules
$37.00extra 10% off with Subscribe & Save

Ritual
Essential for Women Postnatal Multivitamin - Citrus
60 capsules
$44.99extra 20% off with Subscribe & Save

Ritual
Essential for Women Prenatal Multivitamin - Citrus
60 capsules
$44.99extra 20% off with Subscribe & Save