
Ortho Molecular Products
Probiotic 225 by Ortho Molecular Products
15 packets · 15-day supply
High-Potency Probiotics for Digestive and Immune Health$99.29
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Corn Free·Yeast Free·Dairy Free·Milk Free·
Ortho Molecular Products Probiotic 225 overview
If you’re searching for the best probiotic after antibiotics, this 225 billion CFU packet fits that use. A short course makes sense after broad-spectrum antibiotics, during travel-related diarrhea, or when your bowel habits swing after a gut infection. It’s also reasonable if stool testing shows low diversity on a microbiome profile or borderline beneficial species, though labs aren’t required. For chronic constipation or loose stools, many see steadier patterns within 1 to 2 weeks. This is a repletion-level dose; for long-term maintenance, most people step down to a lower-CFU probiotic.
High-dose probiotics crowd out opportunists, compete for nutrients, and restore fermenters that make short-chain fatty acids (fuel for the gut lining). The large CFU load (colony-forming units, a count of live organisms) helps re-seed quickly after a disruption. In practice, people notice less gas from putrefaction and improved stool form as these microbes acidify the colon and reinforce the mucosal barrier. Don’t expect it to treat inflammatory bowel disease; effects on fecal calprotectin (a gut inflammation marker) are inconsistent and this isn’t a stand-alone therapy.
Mix one packet into a cold beverage once daily, ideally with food for better tolerance. If you’re on antibiotics, separate the probiotic by at least 2 to 3 hours. For post-antibiotic repletion, clinicians often use a daily packet for 1 to 2 weeks, then transition to a lower dose. Expect mild bloating in the first few days; it usually settles as the flora adjusts.
Avoid if you’re severely immunocompromised, have a central venous catheter, are in intensive care, or have a history of probiotic-related bloodstream infection. If you have severe pancreatitis or short bowel, discuss with your specialist first. Marked bloating from suspected small intestinal bacterial overgrowth can flare with high CFU; start lower or address overgrowth before repleting. Pregnancy: run high-dose use by your obstetric clinician.
Frequently asked questions
How long does a high-dose probiotic take to work?
Bowel habit changes often show up within 3 to 7 days, with steadier results by 1 to 2 weeks. If nothing changes after two weeks, reconsider dose, timing with meals, or whether a different strain mix is a better fit.
Can I take this probiotic with antibiotics?
Yes, but separate by 2 to 3 hours so fewer organisms are killed on contact. Continue for 1 to 2 weeks after finishing antibiotics to help replete. If you’re on multiple antibiotics, confirm with your prescriber.
Do more CFUs mean a better probiotic?
Higher CFU helps after big disruptions like antibiotics or acute diarrhea. For day-to-day upkeep, lower CFU products often maintain results. Strain quality and survivability matter as much as the number.
Should I refrigerate this probiotic powder?
Store as labeled; most modern powders are shelf-stable to expiration if kept cool and dry. Avoid heat, moisture, and light. Do not mix into hot liquids, which can kill the bacteria.
Can a probiotic cause gas or bloating?
Yes, transient gas or mild bloating is common for a few days as the microbiome shifts. Taking with food and adequate fluids helps. If symptoms persist beyond two weeks or are severe, stop and reassess.
Is this probiotic safe during pregnancy or breastfeeding?
Probiotics are generally considered safe, but high-dose use should be cleared with your obstetric clinician, especially if you have medical complications or immune issues.
Does a probiotic help with inflammation markers like hs-CRP?
Effects on hs-CRP (a blood marker of systemic inflammation) are modest and inconsistent. Choose probiotics for gut symptoms or after antibiotics, not as a primary anti-inflammatory strategy.
How to take it & ingredients
Suggested use: Mix 1 packet into 8 oz of a cold beverage of your choice or as recommended by your health care professional. Consume daily.
Active ingredients
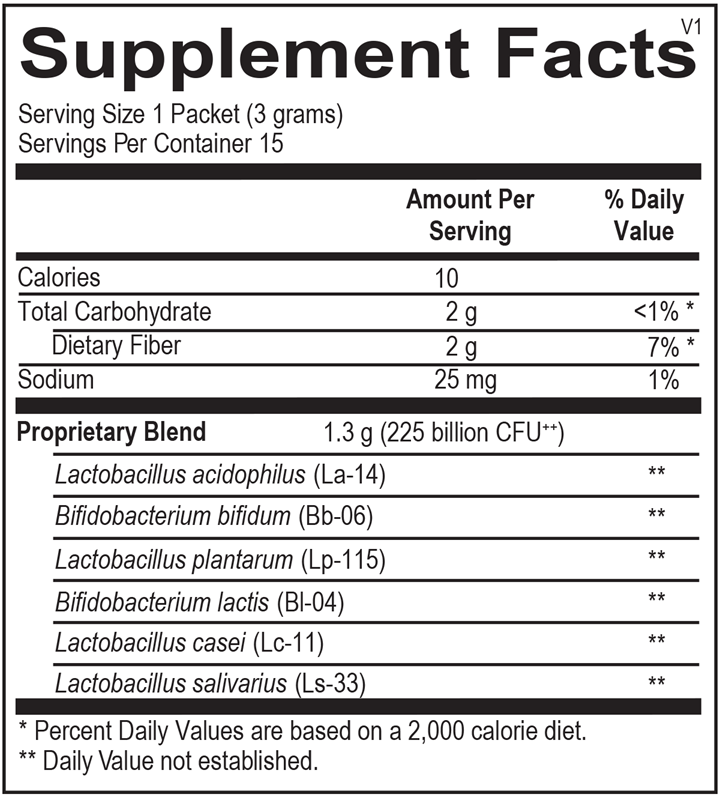
1 packet = 3 grams per serving · 15 servings
▼
Proprietary Probiotic Blend
225 billion CFU, 1.3 gram
Lactobacillus acidophilus (La-14)
-
Lactobacillus plantarum (Lp-115)
-
Bifidobacterium lactis (BI-04)
-
Lactobacillus salivarius (Ls-33)
-
Lactobacillus casei (Lc-11)
-
Bifidobacterium bifidum (Bb-06)
-
Other ingredients: Larch Arabinogalactan (FiberAid), Silicon Dioxide
Certifications
Benefits
Warnings
Customers also considered

Thorne
Bacillus Coagulans
60 capsules
$33.00extra 10% off with Subscribe & Save

Thorne
Complete Biotic
30 packets
$46.00extra 10% off with Subscribe & Save
Dr. Mercola
Complete Probiotics 70 Billion CFU
30 capsules
$46.99extra 19% off with Subscribe & Save
Garden of Life
Dr. Formulated Probiotics Mens Daily Care
30 capsules
$45.99extra 20% off with Subscribe & Save