

Ortho Molecular Products
Reacted Cal-Mag by Ortho Molecular Products
180 capsules · 90-day supply
Essential Calcium and Magnesium for Bone and Muscle Support$75.54
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegetarian·Gluten Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Reacted Cal-Mag overview
If your Vitamin D, 25-Hydroxy is low-normal and your diet is light on dairy, leafy greens, or nuts, a calcium magnesium supplement is a practical way to cover the two minerals bones use most. It also fits people with nighttime calf cramps or frequent muscle tightness, and those on proton pump inhibitors for reflux who often run low on magnesium. If you’re tracking bone density with a DEXA scan (the X‑ray that measures bone strength), pair this with adequate vitamin D and protein for meaningful results.
Calcium is the structural mineral in bone, while magnesium helps convert vitamin D to its active form and keeps parathyroid hormone (the signal that pulls calcium from bone) in a healthy range. In muscle, calcium triggers contraction and magnesium allows relaxation, which is why getting both in balance can ease cramping. Phosphorus is the other half of hydroxyapatite, the crystal that hardens bone. Real-world fracture reduction is most consistent when calcium and magnesium are taken with vitamin D in those who are genuinely low.
Follow the label’s split dosing: 1–2 capsules three times daily with meals. Minerals absorb better in divided doses, and calcium uptake levels off if you take a large amount at once. If you also take iron or levothyroxine (thyroid medication), separate by at least 4 hours. Many people put one dose at dinner since magnesium can feel calming in the evening.
Antibiotics in the tetracycline or fluoroquinolone families bind minerals; separate by 6 hours. Bisphosphonates for osteoporosis also need separation by several hours. Thiazide diuretics raise blood calcium, so avoid extra calcium unless your clinician is monitoring. Loop diuretics increase magnesium loss, which can make this more useful. Check Magnesium, RBC (a red blood cell magnesium test) and PTH if cramps or bone turnover remain an issue.
Skip high-dose calcium if you have a history of high blood calcium, overactive parathyroid, or sarcoidosis, and avoid magnesium supplements in advanced kidney disease unless supervised. If you form kidney stones, take calcium with meals, not between, and discuss total intake with your clinician. Constipation from calcium or loose stools from magnesium are signs to adjust the dose or timing.
Frequently asked questions
How long does a calcium magnesium supplement take to help cramps?
If cramps are related to low magnesium, improvement often shows within 1–2 weeks. For stubborn cases, give it 4 weeks and check Magnesium, RBC to confirm repletion. Persistent cramps despite normal labs warrant a medical workup.
Should I take calcium and magnesium with food or on an empty stomach?
With food is best. Stomach acid and meal-related signals improve mineral absorption, and taking with meals reduces gastrointestinal side effects like nausea or loose stools.
Can I take calcium magnesium with vitamin D and K2?
Yes. Vitamin D improves calcium absorption, and K2 helps direct calcium into bone. Check Vitamin D, 25-Hydroxy after 8–12 weeks to verify you’re in a healthy range before relying on lower maintenance doses.
Does calcium magnesium cause constipation or diarrhea?
Calcium can constipate some people, while magnesium can loosen stools. If you get constipated, increase fluids, add fiber, or reduce the calcium timing. If stools are too loose, move a dose earlier or reduce the total magnesium.
Is a calcium magnesium supplement safe with thyroid medication?
It’s fine if you separate doses. Minerals bind levothyroxine and block absorption. Take thyroid medication on an empty stomach and wait at least 4 hours before taking calcium or magnesium.
Will a calcium magnesium supplement improve bone density by itself?
It helps only as part of a broader plan. The biggest gains come when low vitamin D is corrected, protein intake is adequate, and you do regular resistance and impact training. Recheck bone density on a DEXA every 1–2 years.
Can I take calcium magnesium if I have kidney stones?
Possibly, but timing matters. Taking calcium with meals can reduce oxalate absorption in people with calcium oxalate stones. Avoid large between-meal doses and discuss total calcium intake with your clinician.
How to take it & ingredients
Suggested use: 1-2 capsules three times per day or as recommended by your health care professional.
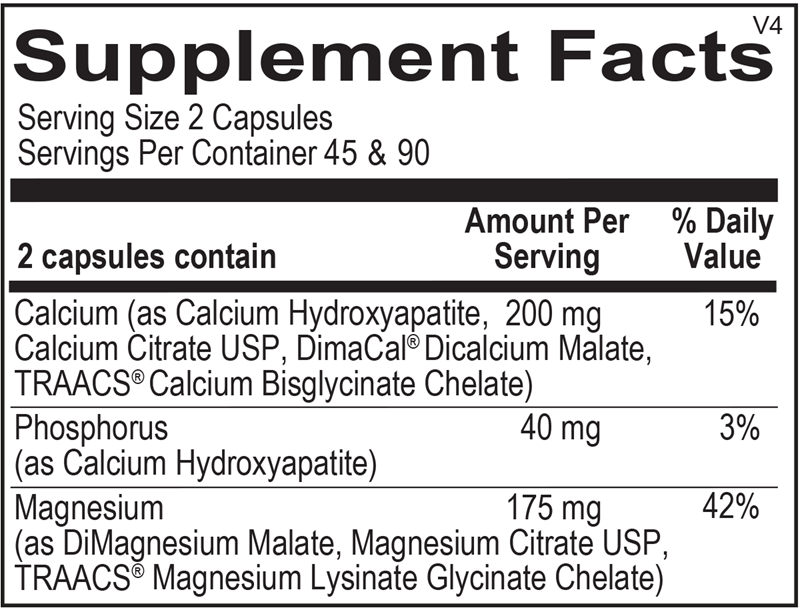
Active ingredients
2 capsules per serving · 90 servings
Calcium
200 mg
Phosphorus
40 mg
Magnesium
175 mg
Other ingredients: Microcrystalline Cellulose, Hypromellose, Stearic Acid, Silicon Dioxide, Magnesium Stearate
Certifications
Benefits
Warnings

