

Ortho Molecular Products
Reacted Cal-Mag by Ortho Molecular Products
90 capsules · 45-day supply
Essential Calcium and Magnesium for Bone and Muscle Support$47.34
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegetarian·Gluten Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Reacted Cal-Mag overview
If you get little dairy or fortified plant milks, or you’re post‑menopausal with a low Vitamin D, 25-Hydroxy level, a calcium magnesium supplement helps fill the mineral gap for bone and muscle. It’s also useful if your Magnesium, RBC is low, you train hard and cramp, or you’re repleting vitamin D (magnesium is a cofactor for its activation). People on long-term proton pump inhibitors often run low on magnesium and may benefit. If your diet already provides ample calcium, use this mainly for the magnesium.
Calcium is the structural mineral for bone, while magnesium helps muscles relax after contraction and stabilizes electrical signaling in nerves and the heart. Phosphorus pairs with calcium in hydroxyapatite (the mineral grid of bone) and is central to ATP, the cell’s energy currency. Together they influence parathyroid hormone (the signal that pulls calcium from bone), so steady, split dosing supports bone turnover balance. Taking calcium with meals also binds dietary oxalate, which can lower calcium‑oxalate stone risk in people prone to stones.
The label suggests 1–2 capsules three times daily. In practice, split doses with meals improve absorption and are gentler on the gut. Aim to get most calcium from food, then use this to cover the remaining 200–600 mg/day gap; the magnesium here functions as a meaningful daily intake for many adults. Pairing with vitamin D3 is reasonable if your Vitamin D, 25-Hydroxy is low. Expect muscle cramp improvements within days to weeks; bone outcomes are measured over months and on DXA scans.
Separate calcium magnesium from levothyroxine, iron, zinc, and antibiotics like doxycycline or ciprofloxacin by at least 2–4 hours to avoid binding. If you take a bisphosphonate for osteoporosis, take that on an empty stomach and minerals later. Use caution or avoid without supervision if you have chronic kidney disease, a history of high calcium, hyperparathyroidism, or sarcoidosis. On thiazide diuretics (hydrochlorothiazide), extra calcium can push blood calcium higher—ask your clinician. For calcium‑oxalate stone formers, take calcium with meals, not between.
Frequently asked questions
When should I take a calcium magnesium supplement?
Take split doses with meals for better absorption and fewer GI side effects. Avoid taking it at the same time as thyroid medication, iron, zinc, or certain antibiotics; separate by 2–4 hours.
How long does calcium magnesium take to work?
Muscle cramp frequency can improve within days to a few weeks. Bone effects are slow; think months to years and track with DXA scans and, if needed, bone turnover markers ordered by your clinician.
Can I take calcium magnesium with vitamin D or K2?
Yes. Vitamin D helps you absorb calcium, and magnesium helps activate vitamin D. Vitamin K2 directs calcium into bone. If your Vitamin D, 25-Hydroxy is low, pairing makes sense under guidance.
Does calcium magnesium cause constipation or stomach upset?
Calcium can constipate some people, while magnesium tends to loosen stools. Taken together with meals, most tolerate it well. If you get constipated, increase fluids, fiber, and consider lowering the calcium dose.
Is calcium magnesium safe if I’ve had kidney stones?
For calcium‑oxalate stone formers, taking calcium with meals can actually reduce oxalate absorption. Avoid large between‑meal calcium boluses and speak with your urologist about your specific stone chemistry.
Does calcium magnesium interfere with thyroid medication?
Yes. Minerals bind levothyroxine and reduce absorption. Take thyroid medication on an empty stomach and wait at least 4 hours before taking calcium or magnesium.
Can I take this with blood pressure or heart medications?
Most blood pressure drugs are fine, but thiazide diuretics (like hydrochlorothiazide) can raise blood calcium. Check labs periodically and ask your clinician before adding extra calcium.
How to take it & ingredients
Suggested use: 1-2 capsules three times per day or as recommended by your health care professional.
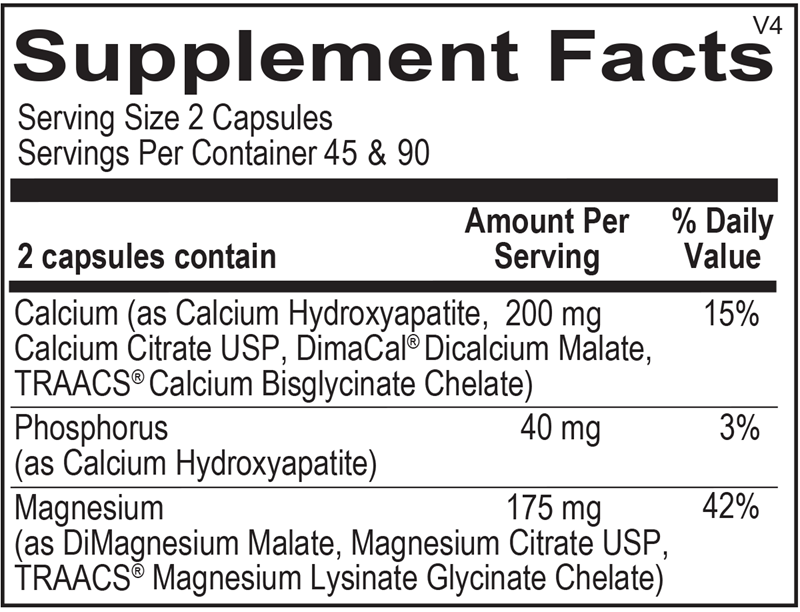
Active ingredients
2 capsules per serving · 45 servings
Calcium
200 mg
Phosphorus
40 mg
Magnesium
175 mg
Other ingredients: Microcrystalline Cellulose, Hypromellose, Stearic Acid, Silicon Dioxide, Magnesium Stearate
Certifications
Benefits
Warnings

