

Ortho Molecular Products
Vitamin K2 with D3 by Ortho Molecular Products
30 capsules · 30-day supply
Essential Vitamins for Bone and Immune Health Support$31.02retail
Add to cart for 10% off
Purchase option
10% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Gluten Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Vitamin K2 with D3 overview
If your Vitamin D, 25-Hydroxy is low or in the lower end of normal and you get little sun, this vitamin K2 with D3 fits. The 5,000 IU D3 here is a higher daily dose, useful for darker-skinned adults at northern latitudes, indoor workers, and post-menopausal women focused on bone density. It also makes sense if you want K2 for calcium handling and your diet is light on fermented foods like natto. If your vitamin D level is already solid, this is maintenance-to-high, so re-test in 8–12 weeks and consider stepping down.
D3 raises calcium absorption from the gut and helps keep parathyroid hormone (the signal that pulls calcium from bone) in check. K2 in the MK-7 form activates osteocalcin (a bone protein that locks calcium into the bone matrix) and matrix Gla protein (a protein that keeps calcium out of arteries). MK-7 has a longer half-life than K1 or MK-4, so it keeps these proteins active through the day. In practice, the pair directs absorbed calcium toward bone and away from soft tissues.
Take one capsule daily with a meal that contains fat for best absorption. Consistency matters more than time of day. This is often enough to raise Vitamin D, 25-Hydroxy within 8–12 weeks; recheck labs and adjust. If you’re already on separate D3, avoid doubling up. You don’t need to add calcium unless your dietary intake is low, and excess calcium supplements can be counterproductive.
Skip K2 if you use warfarin (Coumadin), a vitamin K–antagonist blood thinner, unless your prescriber is closely managing your dose. Direct oral anticoagulants like apixaban and rivaroxaban don’t interact with vitamin K. High-dose D3 is not ideal with a history of high blood calcium, recurrent kidney stones, sarcoidosis, or untreated overactive parathyroid. Fat-blocking drugs (orlistat) and bile acid binders (cholestyramine) reduce absorption; separate by several hours.
Frequently asked questions
How long does vitamin K2 with D3 take to work?
For vitamin D, most people see a rise in Vitamin D, 25-Hydroxy within 8–12 weeks. K2’s activation of osteocalcin and matrix Gla protein occurs within weeks, but changes in bone density take months and require adequate protein, calcium, and resistance training.
Should I take vitamin K2 with D3 with food?
Yes. Both are fat-soluble, so a meal with some fat improves absorption. Taking it at the same time daily helps with consistency. Morning or evening is fine—pick the time you won’t forget.
Is MK-7 better than MK-4 for K2?
MK-7 stays in the body longer than MK-4, keeping vitamin K–dependent proteins active throughout the day at low microgram doses. MK-4 is shorter-acting and often used in much higher milligram doses. For daily convenience, MK-7 is practical.
Can I take vitamin K2 with D3 if I’m on blood thinners?
Do not use K2 with warfarin (Coumadin) unless your prescriber adjusts dosing, because vitamin K changes its effect. Newer blood thinners like apixaban or rivaroxaban don’t rely on vitamin K and generally don’t interact.
Do I need extra calcium with vitamin K2 and D3?
Not automatically. Aim for adequate dietary calcium first. If intake is low, a modest supplement can help, but more is not better. K2 and D3 help direct calcium use; they don’t require high-dose calcium.
What labs should I check while taking vitamin K2 with D3?
Check Vitamin D, 25-Hydroxy after 8–12 weeks. If you have a history of high blood calcium or kidney stones, also monitor Calcium and consider parathyroid hormone with your clinician. Specialized K2 markers exist but aren’t routine.
Is vitamin K2 with D3 safe for kidney stone formers?
Use caution. High vitamin D can raise calcium absorption, which may matter in certain stone types. Work with a clinician, monitor Calcium and urine studies if you have a stone history, and keep hydration and diet on point.
How to take it & ingredients
Suggested use: Take 1 capsule per day or as recommended by your health care professional.
Active ingredients
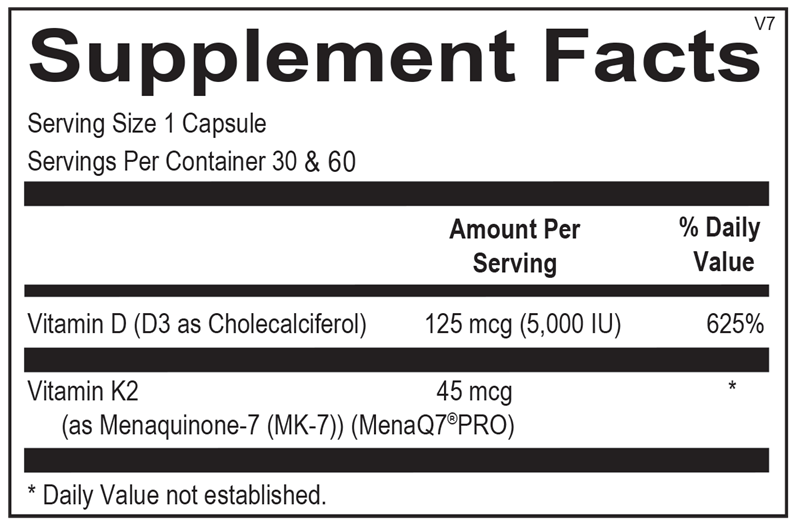
1 capsule per serving · 30 servings
Vitamin K2
As Menaquinone-7 (MK-7) (MenaQ7® PRO)
As Menaquinone-7 (MK-7) (MenaQ7® PRO)
45 mcg
Vitamin D
D3 as Cholecalciferol
D3 as Cholecalciferol
125 mcg, 5000 IU
Other ingredients: Microcrystalline Cellulose, Hypromellose (Natural Vegetable Capsule), Magnesium Stearate, Silicon Dioxide, Stearic Acid
Certifications
Benefits
Warnings
Customers also considered

Ortho Molecular Products
K-FORCE
60 capsules
$60.33
Add to cart for lower price

Ortho Molecular Products
K-FORCE MAX
30 capsules
$44.79
Add to cart for lower price

Ortho Molecular Products
Liquid Vitamin D3 with K2
30 milliliters
$52.00
Add to cart for lower price

NBI
Osteo-K Minis
120 capsules
$65.99
Add to cart for lower price