

Ortho Molecular Products
Vitamin K2 with D3 by Ortho Molecular Products
60 capsules · 60-day supply
Essential Vitamins for Bone and Heart Health Support$47.01
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Vitamin K2 with D3 overview
This fits adults using vitamin K2 with D3 to shore up bone strength while keeping calcium where it belongs. It’s a smart pick if your Vitamin D, 25-Hydroxy is in the lower part of the normal range, you get little sun, have darker skin, or live at northern latitudes. Post‑menopausal women and long‑term dairy‑avoidant eaters often benefit. The D3 here is a repletion‑level dose for many; the MK‑7 dose is conservative, good for maintenance if your diet includes leafy greens or fermented foods.
D3 raises calcium absorption and helps normalize parathyroid hormone (the signal that pulls calcium from bone). K2 as MK‑7 activates osteocalcin (the protein that locks calcium into bone) and matrix Gla protein (a protein that helps keep calcium out of artery walls). Together, they drive calcium toward your skeleton and away from soft tissues. In practice, PTH can improve within weeks; meaningful bone changes take months of steady intake and weight‑bearing exercise.
Take one capsule daily with a meal that contains fat for better absorption. If your Vitamin D, 25-Hydroxy is low, this 5,000 IU D3 level is commonly used for 8–12 weeks before retesting, then many step down. If your level is already adequate, consider less frequent dosing of D3 or a lower‑dose D3 under clinician guidance. Track calcium and PTH if you’re on long‑term higher‑dose D3.
Skip K2 supplements if you take warfarin or other vitamin K–antagonist blood thinners unless your prescriber adjusts your dose. Use caution with high‑dose D3 if you have a history of high calcium, kidney stones, sarcoidosis, or hyperparathyroidism, and monitor calcium. If you also take calcium, keep total daily intake reasonable and prioritize food sources; more calcium is not always better.
Frequently asked questions
Is 5,000 IU of vitamin D3 safe to take daily?
For many adults, 5,000 IU daily is used short term to raise low Vitamin D, 25-Hydroxy, then tapered. If your level is already adequate, this can overshoot. Recheck labs in 8–12 weeks and discuss the right maintenance dose with your clinician.
Do I need to take vitamin K2 with D3 with food?
Yes, take it with a meal that contains fat. Both D3 and K2 are fat‑soluble, and absorption is better when taken with dietary fat like olive oil, eggs, or avocado.
How long does vitamin K2 with D3 take to work for bones?
You can see PTH (parathyroid hormone) improvements within weeks, but bone changes take longer. Expect months for shifts in bone turnover markers and years for measurable differences on a DEXA scan, alongside strength training and adequate protein.
Can I take vitamin K2 if I’m on warfarin?
Not without medical supervision. Warfarin works by blocking vitamin K recycling, so adding K2 can counteract your medication. Talk to your prescriber before using any K supplement.
Should I pair vitamin K2 with calcium?
Only if your dietary calcium is low. Many adults meet needs with food. If you add a supplement, keep the dose moderate and split with meals. Track calcium and Vitamin D, 25-Hydroxy if using long term.
What’s the difference between MK-7 and MK-4?
MK‑7 stays in the blood longer, so lower daily doses can maintain activity. MK‑4 has a shorter half‑life and is often dosed multiple times per day or at higher amounts. This formula uses MK‑7 for once‑daily convenience.
Which labs should I check while taking this?
Vitamin D, 25-Hydroxy is the primary check. Consider calcium and PTH to ensure you’re not overshooting on D3. Your clinician may track bone turnover markers during longer courses.
Is vitamin K2 with D3 okay if I’ve had kidney stones?
Use caution with higher‑dose D3 if you form calcium stones. Ensure good hydration, avoid excessive calcium supplements, and monitor calcium with your clinician.
How to take it & ingredients
Suggested use: Take 1 capsule per day or as recommended by your health care professional.
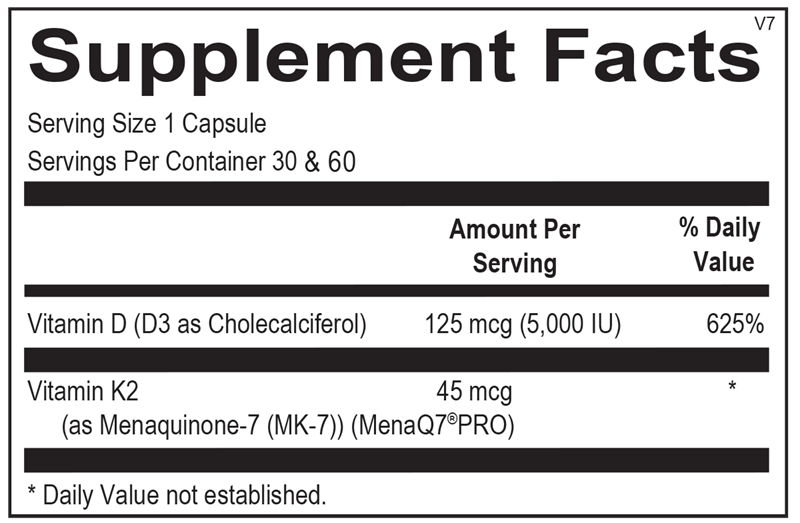
Active ingredients
1 capsule per serving · 60 servings
Vitamin K2
As Menaquinone-7 (MK-7) (MenaQ7® PRO)
As Menaquinone-7 (MK-7) (MenaQ7® PRO)
45 mcg
Vitamin D
D3 as Cholecalciferol
D3 as Cholecalciferol
125 mcg, 5000 IU
Other ingredients: Microcrystalline Cellulose, Hypromellose (Natural Vegetable Capsule), Magnesium Stearate, Silicon Dioxide, Stearic Acid
Certifications
Benefits
Warnings
Customers also considered

Life Extension
Bone Restore Calcium Supplement with Vitamin K2
120 capsules
$24.99extra 20% off with Subscribe & Save

Ortho Molecular Products
K-FORCE
60 capsules
$60.33extra 10% off with Subscribe & Save

Ortho Molecular Products
K-FORCE MAX
30 capsules
$44.79extra 10% off with Subscribe & Save

Ortho Molecular Products
Liquid Vitamin D3 with K2
30 milliliters
$52.00extra 10% off with Subscribe & Save