


Thorne
Vitamin K 6090 mcg by Thorne
60 capsules · 60-day supply
Supports Healthy Bones and Cardiovascular Function$31.00
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Dairy Free·Milk Free
Thorne Vitamin K overview
If you’re aiming to keep calcium in bone and out of arteries, a vitamin K2 supplement is worth considering. It fits post‑menopausal women, adults with low vegetable intake, and anyone taking vitamin D who wants the cofactor that activates bone proteins. It’s also useful if you have fat‑malabsorption (celiac, inflammatory bowel disease), use fat‑blocking drugs like orlistat or bile acid binders such as cholestyramine, or your diet is mostly ultra‑processed and light on leafy greens.
Vitamin K activates proteins by adding a carboxyl group, which lets them bind calcium where it belongs. K1 focuses on liver clotting factors, while K2 (MK‑4 and MK‑7) activates osteocalcin (a bone protein that helps lock calcium into the matrix) and matrix Gla‑protein (a vessel‑wall protein that helps keep calcium from depositing in arteries). MK‑7 has a longer half‑life, giving steadier activation; MK‑4 is the form most tissues use. Together they improve vitamin K–dependent protein status within weeks, while bone and arterial effects accrue over months.
Take one capsule daily with a meal that contains fat; vitamin K is fat‑soluble and absorbs better with food. Pairing it with vitamin D3 and your calcium dose is reasonable because these nutrients work on the same pathways. Expect lab shifts in vitamin K–dependent protein status within 4 to 12 weeks, but changes in bone density or arterial calcification take longer. This is a high‑potency blend, so daily consistency matters more than timing.
If you take warfarin (a vitamin K–antagonist blood thinner), do not start or stop vitamin K without your prescriber; it will change your INR (the clotting time test) and your dose will need adjustment. Long‑term broad‑spectrum antibiotics can lower vitamin K made by gut bacteria, making supplementation temporarily more relevant. Orlistat and cholestyramine reduce absorption—separate by at least 4 hours. For those on newer blood thinners not targeting vitamin K, routine dietary vitamin K is fine, but ask your clinician before high‑dose use.
K2 vs K1: K1 mainly supports clotting in the liver; K2 (MK‑4, MK‑7) turns on proteins in bone and arteries. Combining K2 with vitamin D, and adequate calcium and magnesium, is practical because they act on the same bone‑building system. Evidence for arterial calcification reduction is mixed; what’s clear is improved activation of K‑dependent proteins, which you’ll see within weeks, while structural changes take months.
Frequently asked questions
Do I need vitamin K2 if I already take vitamin D?
Often, yes. Vitamin D raises calcium absorption, and vitamin K2 activates proteins that use that calcium in bone and keep it out of arteries. Many clinicians pair them. If your Vitamin D, 25-Hydroxy is low, correct that too; K2 is not a substitute for vitamin D.
How long does vitamin K2 take to work for bones?
Activation of K‑dependent proteins improves within 4–12 weeks. Detectable changes in bone density usually take 6–12 months. Use it consistently, alongside adequate calcium, vitamin D, and resistance exercise, and track progress with periodic DEXA scans rather than expecting quick changes.
Is vitamin K2 safe with blood thinners?
With warfarin, no—don’t start or change vitamin K without your prescriber, as it will alter your INR and warfarin dose requirements. With newer blood thinners that do not target vitamin K, interactions are less likely, but discuss any high‑dose supplement with your clinician first.
Should I take vitamin K2 with food or on an empty stomach?
Take it with food that contains fat. Vitamin K is fat‑soluble and absorbs better with a meal. If you use fat‑blocking medications like orlistat or bile acid binders, separate doses by at least 4 hours to avoid reduced absorption.
What’s the difference between MK-4 and MK-7 in vitamin K2?
MK‑4 is the tissue‑active form used widely in the body; MK‑7 stays in the blood longer, giving steadier activation of K‑dependent proteins. A blend covers both kinetics. MK‑7 is often used for once‑daily dosing; MK‑4 has a history of higher‑dose use in bone research.
Can vitamin K2 cause side effects?
In healthy adults not on warfarin, side effects are uncommon. Occasional reports include mild gastrointestinal upset when taken on an empty stomach. The main risk is interaction with warfarin, which can change your INR. Take with food to improve tolerance.
Who should avoid vitamin K supplements?
Anyone on warfarin should avoid unsupervised vitamin K. Use caution with active liver disease, a history of unexplained clotting, or known fat‑malabsorption until you’ve discussed dosing with your clinician. Pregnancy and breastfeeding: stick to dietary intake unless advised by your obstetric provider.
How to take it & ingredients
Suggested use: Adults take one capsule daily, with food, or as directed by your healthcare professional.
Active ingredients
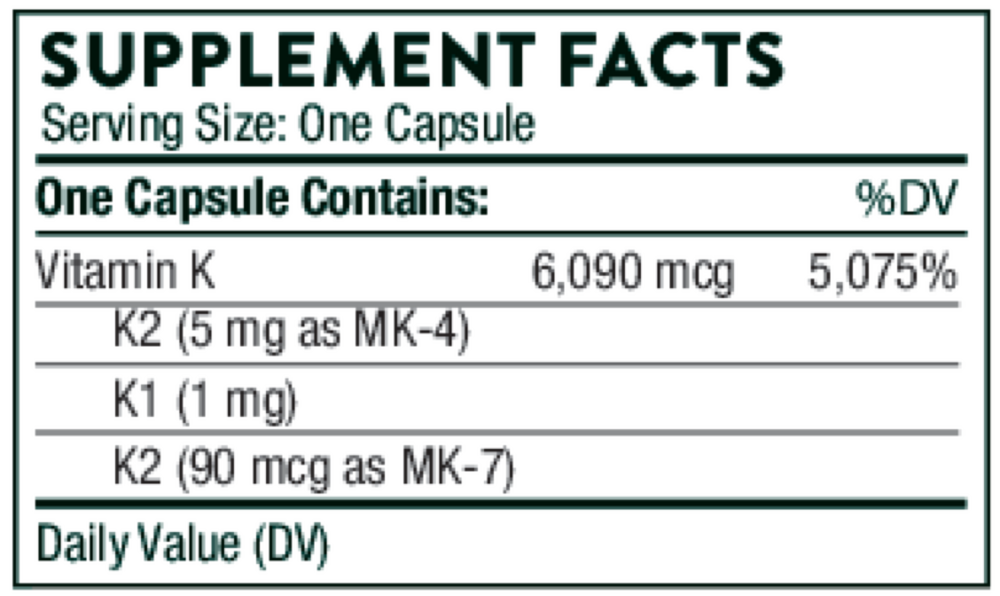
1 capsule per serving · 60 servings
▼
Vitamin K
6090 mcg
Vitamin K1
1000 mcg
Vitamin K2
MK-4
MK-4
5000 mcg
Vitamin K2
MK-7 (MenaQ7®)
MK-7 (MenaQ7®)
90 mcg
Other ingredients: Hypromellose Capsule, Microcrystalline Cellulose, Mixed Tocopherols, Silicon Dioxide
Certifications
Benefits
Warnings

