

VSL#3
High-Potency, Multi-Strain Probiotic 112.5 billion CFU by VSL#3
60 capsules · 60-day supply
Support Digestive Health with 112.5 Billion CFU of Probiotics$74.99
This item is currently out of stockGet notified when this item is back in stock
Practitioner-grade brand3rd-party testedFree shipping $50+
Halal Certified·Kosher·Dairy Free
VSL#3 High-Potency, Multi-Strain Probiotic overview
If you are looking for a high potency probiotic for IBS, this fits adults with frequent bloating, irregular stools, or urgency who want a clinically studied dose. The strongest evidence is as an add-on in irritable bowel syndrome, ulcerative colitis, and pouchitis when guided by a clinician. It is also reasonable after antibiotics or during travel if you have a history of gut flare-ups. Track symptoms and, when relevant, fecal calprotectin (a stool marker of gut inflammation).
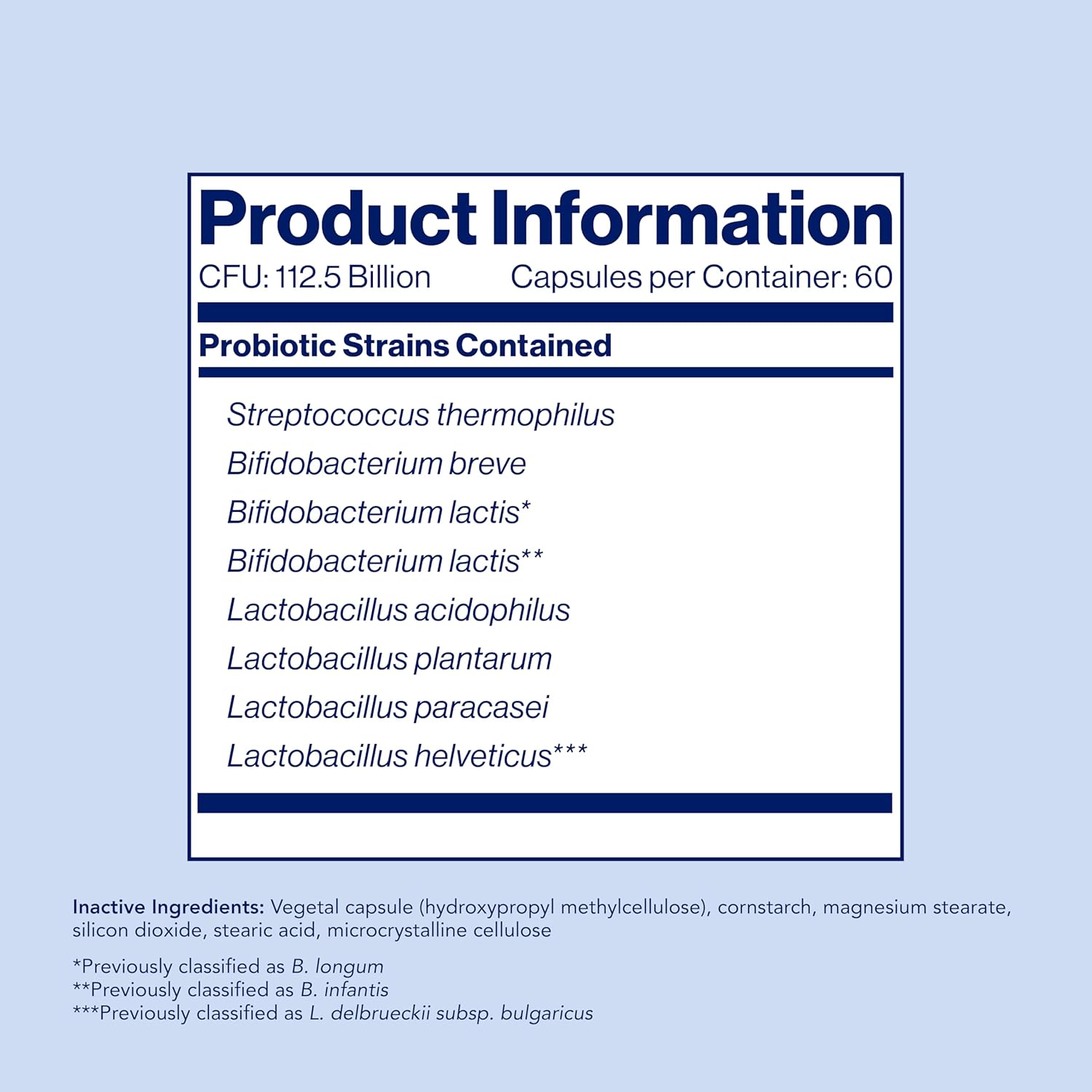
The eight strains here total 112.5 billion CFU (colony-forming units, a count of live bacteria) per capsule. Together they crowd out gas-producing microbes, strengthen the mucosal barrier, and raise short-chain fatty acids like butyrate, the fuel your colon cells prefer. These changes can reduce visceral hypersensitivity (the gut’s tendency to overreact to stretch), ease bloating, and help normalize stool form. In some trials, inflammatory signals such as fecal calprotectin and hs-CRP (a blood marker of inflammation) decreased in responders.
The label allows 1–2 capsules up to four times daily under medical supervision. In practice, start low: 1 capsule daily with food for 3–7 days to limit gas, then increase every few days until you reach your target. Separate from antibiotics by at least 2 hours. Benefits for bloating often appear within 1–2 weeks; bowel pattern and urgency typically need 4–8 weeks. Follow storage instructions closely, as many high-CFU probiotics require refrigeration.
Avoid probiotics if you are severely immunocompromised, have a central venous catheter, or a history of probiotic-related bloodstream infection. Post–bowel surgery, pancreatitis, or critical illness are also times to defer unless your specialist approves. If you have small intestinal bacterial overgrowth diagnosed by breath testing, high-dose probiotics can worsen gas; consider targeted treatment first. Pregnancy and breastfeeding: discuss with your obstetric clinician before starting high-potency products.
Frequently asked questions
How long does a high-potency probiotic take to work?
Bloating and gas often improve within 1–2 weeks. Stool consistency, urgency, and bathroom frequency usually need 4–8 weeks. If nothing changes by 8 weeks at a steady dose, it is reasonable to reassess the plan with your clinician.
Should I take this probiotic with or without food?
Either is acceptable, but taking it with a meal is easier on the stomach and often reduces initial gas. Be consistent with timing day to day. If you are also on antibiotics, separate by at least 2 hours.
Do I need to refrigerate VSL#3 or similar probiotics?
Many high-CFU probiotics are refrigerated to maintain potency. Follow the storage instructions on your bottle. Short room-temperature periods during shipping are usually accounted for by overfilling at manufacture.
Can I open the capsule and mix the powder into food?
Yes, opening and mixing into cool, soft food or a non-hot beverage is fine. Avoid hot liquids, which can kill live bacteria. Take the full contents at once rather than splitting unevenly across doses.
Is a high-potency probiotic safe with immunosuppressants or biologics?
Often yes, but check with your prescribing specialist. People who are severely immunocompromised have a higher risk of probiotic bloodstream infection and should avoid live microbes unless specifically cleared.
Can a probiotic help lower fecal calprotectin?
In some responders, stool inflammation markers like fecal calprotectin fall over weeks to months, especially when used alongside standard therapy. Not everyone responds, so pair it with objective monitoring and clinician oversight.
What side effects should I expect at first?
Temporary gas, bloating, or mild cramping are common in the first week and usually settle as your microbiome adapts. Slower titration and taking with food help. Stop and seek care for fever, severe pain, or persistent worsening.
Can I take this if I have SIBO?
If you have small intestinal bacterial overgrowth, high-dose probiotics can aggravate gas and bloating. Treat SIBO first under clinician care, then consider reintroducing a probiotic at a low dose while monitoring symptoms.
How to take it & ingredients
Suggested use: Use under medical supervision. Usual adult dosage: 1–2 capsules, as needed, up to four times daily.
Active ingredients
1 capsule per serving · 60 servings
▼
Probiotics
112.5 billion CFU
Bifidobacterium infantis
-
Lactobacillus acidophilus
-
Lactobacillus delbrueckii subsp. bulgaricus
-
Lactobacillus paracasei
-
Lactobacillus plantarum
-
Streptococcus thermophilus
-
Bifidobacterium breve
-
Bifidobacterium longum
-
Other ingredients: Hydroxypropyl methylcellulose, Cornstarch, Magnesium stearate, Silicon dioxide, Stearic acid, Microcrystalline cellulose
Certifications
Benefits
Warnings
Customers also considered

Thorne
Bacillus Coagulans
60 capsules
$33.00extra 10% off with Subscribe & Save

Thorne
Complete Biotic
30 packets
$46.00extra 10% off with Subscribe & Save
Dr. Mercola
Complete Probiotics 70 Billion CFU
30 capsules
$46.99extra 19% off with Subscribe & Save

SmartyPants
Digestive Probiotic & Prebiotic Grape
60 gummies
$36.99extra 19% off with Subscribe & Save