
Codeage
ADK Vitamins+ by Codeage
180 capsules
Comprehensive Support for Bone Health and Immune Function$XX.XX$44.99retail
This item is currently out of stockGet notified when this item is back in stock
20% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Codeage ADK Vitamins+ overview
If your Vitamin D, 25-Hydroxy is on the low side or you rarely get midday sun, a vitamin D3 and K2 combo fits. It also suits adults who eat few leafy greens (low vitamin K intake) or who take calcium but want it going into bone, not soft tissue. The added vitamin A helps if your diet is light on liver, eggs, or full-fat dairy. For established deficiency, you’ll often need a higher standalone D3 repletion plan first, then step down to a combo.
D3 raises calcium absorption from the gut and helps normalize parathyroid hormone (PTH, the signal that pulls calcium from bone). K2 activates osteocalcin and matrix Gla protein (vitamin K–dependent proteins that load calcium into bone and keep it out of arteries). Vitamin A modulates bone turnover and keeps barrier tissues healthy, but too much A can counter D-driven signaling. Together, D3 and K2 improve calcium handling; in responders you’ll see PTH drift down with stable Calcium within 4 to 12 weeks.
Take one capsule daily with a meal that contains fat for better absorption. If your Vitamin D, 25-Hydroxy is meaningfully low, a higher-dose D3 phase is usually more practical, then switch to this for maintenance. Retest Vitamin D, 25-Hydroxy in 8 to 12 weeks, and consider PTH and Calcium if you’ve needed higher D3. Avoid doubling up with cod liver oil or separate high-dose vitamin A unless a clinician is tracking your total retinol intake.
Skip K2 if you use warfarin (a blood thinner that works by blocking vitamin K), unless your prescriber plans INR checks with a stable, consistent K intake. Avoid extra preformed vitamin A if you’re pregnant or trying to conceive; choose prenatal formulas that use beta-carotene instead. Use caution with a history of high calcium, kidney stones, sarcoidosis, or lymphoma, and loop in your clinician. Heavy alcohol use or liver disease also warrants careful vitamin A management.
Frequently asked questions
Do I need vitamin K2 with vitamin D3?
You don’t strictly need it, but K2 helps activate proteins that steer calcium into bone and away from arteries. If you take D3 or calcium and eat few leafy greens or fermented foods, adding K2 is a practical way to cover that gap.
How long until vitamin D3 and K2 start working?
Most people see Vitamin D, 25-Hydroxy move within 4 to 12 weeks of steady dosing. Effects on PTH and bone turnover follow that timeline. Retest at 8 to 12 weeks, then adjust. True bone-density changes take months to years.
Can I take vitamin D3 and K2 with calcium?
Yes. Taking them with calcium is common, and K2 helps direct where calcium is used. If you already get ample dietary calcium, you may not need a separate calcium pill. Monitor Calcium and discuss long-term dosing with your clinician.
Is the vitamin A in ADK safe to take daily?
For non-pregnant adults with normal liver function, typical daily doses are safe. Total vitamin A adds up from diet and other supplements, so avoid stacking with cod liver oil or separate retinol products. Pregnancy requires avoiding extra retinol.
Does vitamin K2 interfere with blood thinners?
K2 interferes with warfarin, which works by blocking vitamin K recycling. Do not start K2 on warfarin without medical supervision and INR monitoring. K2 does not meaningfully interact with newer anticoagulants, but confirm with your prescriber.
Should I take vitamin D3 and K2 in the morning or at night?
Either is fine. Take it with a meal that contains fat to improve absorption and pick a time you can stick with daily. If D3 affects your sleep, move it earlier in the day, though most people notice no difference.
What side effects should I watch for?
Rarely, high D3 can raise Calcium, causing thirst, constipation, or fatigue. Too much vitamin A can cause headache or nausea. These usually reflect overdoing dose or stacking products. If symptoms occur, stop and check labs with your clinician.
How to take it & ingredients
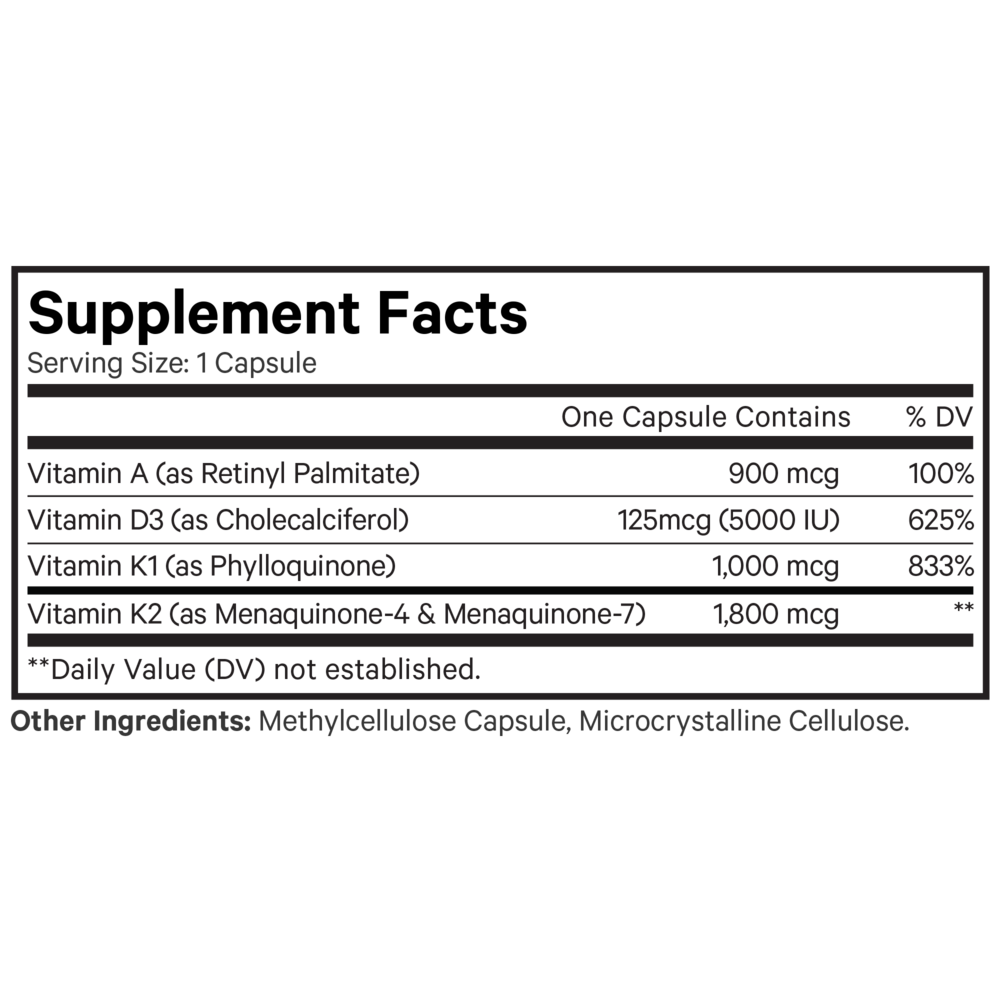
Suggested use: Adults take one capsule daily, with food, or as directed by your healthcare professional.
Certifications
Benefits
Warnings
Customers also considered

Nature’s Way
Alive! Men’s 50+ Ultra Potency
60 tablets
$XX.XX$29.99retail
Add to cart to see your price

Ortho Molecular Products
Alpha Base® Capsules with Iron
240 capsules
$XX.XX$74.31retail
Add to cart to see your price

Ortho Molecular Products
Alpha Base® Capsules without Iron
120 capsules
$XX.XX$46.79retail
Add to cart to see your price
Ortho Molecular Products
Alpha Base® Premier Packs
30 packets
$XX.XX$109.50retail
Add to cart to see your price