
Dr. Mercola
Liposomal Vitamin D3 5000 IU by Dr. Mercola
30 capsules · 30-day supply
Enhanced Absorption of Vitamin D for Immune and Bone Health$21.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free
Dr. Mercola Liposomal Vitamin D3 5000 IU overview
If your Vitamin D, 25-Hydroxy is low or stuck in the lower end despite a basic multivitamin, vitamin D3 5000 IU is a practical step-up. It fits adults with little sun exposure, darker skin, higher body weight, or those on restrictive diets. Liposomal vitamin D3 is also reasonable for people with fat-malabsorption issues who don’t absorb standard softgels well. If your level is only slightly low, this is more than a maintenance dose, so plan to recheck labs and step down once repleted.
Cholecalciferol (vitamin D3) is the same form your skin makes from sunlight, and it raises blood Vitamin D, 25-Hydroxy more reliably than D2. In liposomal vitamin D3, the D3 is wrapped in phospholipids from sunflower lecithin so it mixes with water and fat more easily, which can improve uptake in some people. Adequate D3 increases calcium absorption from the gut and helps restrain parathyroid hormone (the signal that pulls calcium from bone). Take it for bone and metabolic health; the infection-prevention hype did not hold up well in randomized trials.
Take one capsule daily with food as directed by Dr. Mercola, since dietary fat still helps absorption even with a liposomal format. Recheck Vitamin D, 25-Hydroxy after 8–12 weeks and adjust. This dose often suits repletion or higher ongoing needs; once your level is steady, many people transition to a lower maintenance dose. If you also take calcium, separate large doses to avoid stomach upset.
Avoid high-dose vitamin D3 if you’ve had high calcium, recurrent kidney stones, sarcoidosis or other granulomatous disease, or certain lymphomas, unless your clinician is monitoring calcium and Vitamin D, 25-Hydroxy. Thiazide diuretics (blood pressure meds that reduce calcium loss) raise the risk of high calcium when combined with high-dose D3. Orlistat and bile acid sequestrants (fat-blocking drugs) reduce absorption, so take vitamin D3 at a different time.
Frequently asked questions
How long does vitamin D3 5000 IU take to raise levels?
Most adults see a meaningful rise in Vitamin D, 25-Hydroxy within 4–12 weeks. Recheck labs in that window, then adjust the dose down for maintenance once you’re in your target range.
Is liposomal vitamin D3 better absorbed than regular D3?
It can be for some people, especially those with fat-malabsorption. For many healthy adults, taking standard vitamin D3 with a meal works well too. The advantage of liposomal is most relevant when absorption is uncertain.
Should I take vitamin K2 with vitamin D3 5000 IU?
K2 is not required to take with vitamin D3, but some clinicians pair them when calcium intake is high. If you’re on warfarin or have a bleeding disorder, discuss K2 with your clinician first.
Can I take vitamin D3 5000 IU every day long term?
You can if your labs are monitored and stable, but many people step down to a lower maintenance dose once repleted. Check Vitamin D, 25-Hydroxy and calcium periodically to avoid overshooting.
What time of day should I take vitamin D3?
Take vitamin D3 with a meal you reliably eat, often breakfast or lunch. Consistency and taking it with food matter more than the clock.
What are the side effects of too much vitamin D3?
Excess vitamin D3 can raise calcium, causing nausea, constipation, thirst, or kidney stones. If you develop symptoms or your calcium rises on labs, stop and contact your clinician.
Does vitamin D3 interact with medications?
Yes. Thiazide diuretics increase the risk of high calcium when combined with high-dose D3. Orlistat and bile acid sequestrants reduce absorption; separate dosing. Steroids can lower vitamin D levels.
How to take it & ingredients
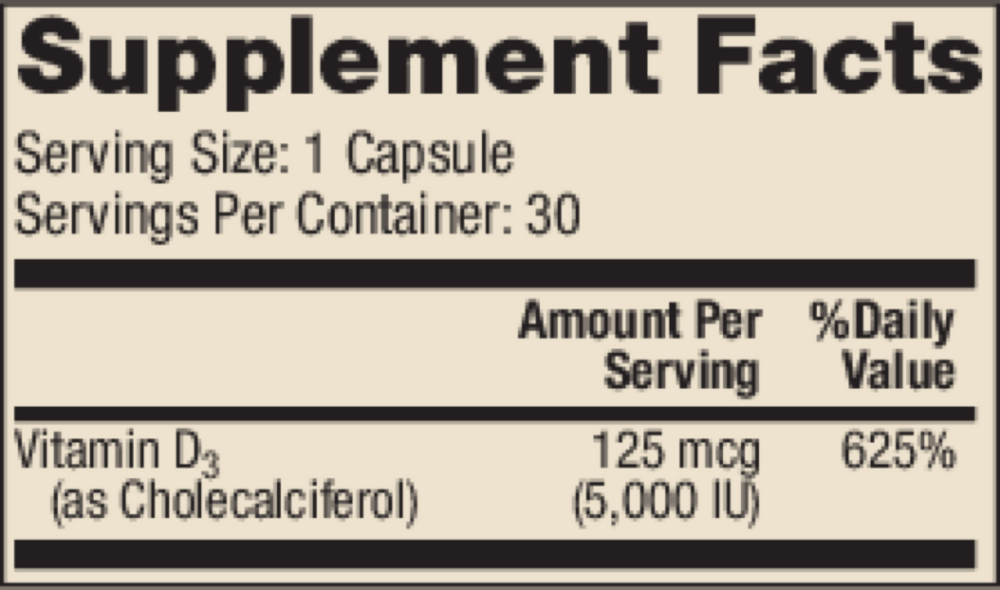
Suggested use: Adults take one capsule daily, with food, or as directed by your healthcare professional.
Active ingredients
1 capsule per serving · 30 servings
Vitamin D
Vitamin D3 (Cholecalciferol)
Vitamin D3 (Cholecalciferol)
5000 IU, 125 mcg
Other ingredients: Sunflower Lecithin, Medium Chain Triglycerides, Hydroxypropyl Methylcellulose Capsule
Certifications
Benefits
Warnings



