



Thorne
D-5,000 by Thorne
60 capsules · 60-day supply
Essential Vitamin D for Bone, Immune, and Mood Support$20.00
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Dairy Free·Milk Free
Thorne D-5,000 overview
If your Vitamin D, 25-Hydroxy is low or stuck in the lower-normal range, vitamin D3 5000 IU is a practical daily dose to move it up within 4 to 12 weeks. It fits darker‑skinned adults, indoor workers, northern latitudes, consistent sunscreen users, and those with higher body weight who often need more to achieve the same blood level. It’s also useful if absorption is limited by celiac disease, bariatric surgery, or fat‑blocking drugs. For steady maintenance once your level is where you want it, many people can step down to a lower dose.
Cholecalciferol (vitamin D3) is the form your skin makes from sunlight and is better at raising blood levels than D2 (ergocalciferol). Your liver and kidneys convert D3 into the active hormone that increases calcium absorption from the gut and regulates bone turnover. Adequate D3 keeps parathyroid hormone (the signal that pulls calcium out of bone) in check. Interest in D for infection soared during COVID, but large randomized trials show little to no prevention effect, so take it to correct a low level, not as an immune panacea.
Take one capsule daily with a meal that contains some fat to improve absorption. Morning or evening both work; consistency matters more than timing. Recheck Vitamin D, 25-Hydroxy after 8 to 12 weeks to see if this dose is still needed. If you already take calcium, keep total calcium intake steady while adjusting D3, and avoid stacking multiple D products unknowingly. Thorne D-5,000 provides a single-ingredient, NSF Certified for Sport option.
Skip high‑dose D3 without medical guidance if you’ve had high calcium, recurrent calcium‑based kidney stones, sarcoidosis or other granulomatous disease (conditions that can overproduce active D), or certain lymphomas. Thiazide diuretics (water pills that raise calcium), high‑dose calcium, and long courses of vitamin A increase the risk of high calcium. Orlistat and cholestyramine reduce absorption; anticonvulsants and chronic steroids increase D breakdown, often requiring lab‑guided dosing.
Frequently asked questions
How long does vitamin D3 5000 IU take to raise my levels?
Most people see a measurable rise in Vitamin D, 25-Hydroxy within 4 to 12 weeks. Recheck at that point and adjust. If levels barely move, consider adherence, taking it with fat, gut absorption issues, interacting meds, or a higher personalized dose under clinician guidance.
Should I take vitamin D3 with food or on an empty stomach?
Take vitamin D3 with a meal that contains fat for better absorption. It’s fat‑soluble, so a snack with eggs, yogurt, avocado, nuts, or olive oil works. Taking it on an empty stomach absorbs less and can lead to smaller changes on follow‑up labs.
Is vitamin D3 5000 IU safe to take every day?
For adults correcting a low Vitamin D, 25-Hydroxy, daily 5000 IU is commonly used short‑term with lab follow‑up. Long‑term use should be guided by repeat labs to avoid excessive levels. If your level is already adequate, a lower maintenance dose is usually sufficient.
What’s the difference between vitamin D2 and D3?
Vitamin D3 (cholecalciferol) raises and sustains blood levels better than D2 (ergocalciferol) in most studies. D3 is the form your skin makes from sunlight. If you’re correcting a low level, D3 is generally the more effective choice unless your clinician specifies D2.
Which medications interact with vitamin D3?
Thiazide diuretics can increase blood calcium when combined with high‑dose D. Orlistat and cholestyramine reduce D absorption. Some anticonvulsants and chronic steroids increase D breakdown. If you use these, coordinate dosing and monitor Vitamin D, 25-Hydroxy and calcium with your clinician.
Can vitamin D3 help immunity or mood?
Correcting a low level is reasonable for general health, but large randomized trials don’t show vitamin D prevents infections. Mood effects are inconsistent; benefits are more likely if you’re deficient. Use labs to guide dosing rather than taking it specifically for mood or colds.
Do I need vitamin K2 with vitamin D3?
Vitamin K2 helps activate proteins that handle calcium, but evidence that adding K2 to D3 prevents fractures or calcification in generally healthy adults is mixed. If you eat little K‑rich foods or take high‑dose D long‑term, discuss K2 with your clinician.
How to take it & ingredients
Suggested use: Take 1 capsule daily or as recommended by your health professional.
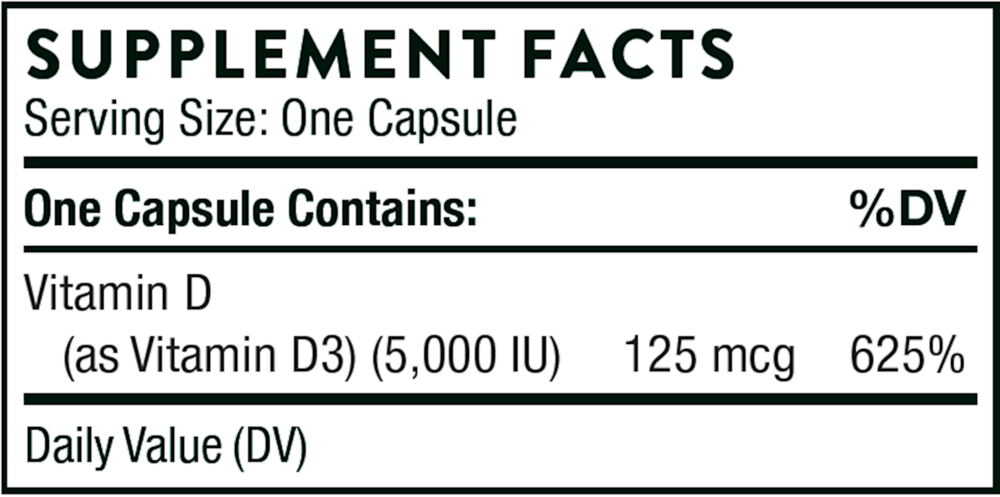
Active ingredients
1 capsule per serving · 60 servings
Vitamin D
Vitamin D3
Vitamin D3
125 mcg, 5000 IU
Other ingredients: Hypromellose Capsule, Leucine, Microcrystalline Cellulose, Silicon Dioxide, Vitamin E (d-Alpha-Tocopheryl)
Certifications
Benefits
Warnings



