


Thorne
D-10,000 by Thorne
60 capsules · 60-day supply
High-Potency Vitamin D3 for Immune and Bone Health Support$26.00
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Dairy Free·Milk Free
Thorne D-10,000 overview
Choose vitamin D3 10,000 IU if your Vitamin D, 25-Hydroxy is low and your clinician wants a short-term repletion plan. It’s a fit after malabsorption (celiac, inflammatory bowel disease, bariatric surgery), for darker‑skinned adults at northern latitudes, consistent sunscreen users, or those on long-term steroids. People with higher body weight often need larger intakes to move levels. This dose is usually for 4–12 weeks, then you step down. If your level is only slightly low, a maintenance dose (1,000–2,000 IU) is usually enough.
Cholecalciferol (vitamin D3) is the form your skin makes from sunlight, and it raises Vitamin D, 25-Hydroxy more reliably than D2 (ergocalciferol). Your liver and kidneys convert D3 into the active hormone that increases calcium absorption from the gut and keeps parathyroid hormone (PTH, the signal that pulls calcium from bone) in check. Adequate D3 maintains bone remodeling balance. Hopes that vitamin D prevents respiratory infections are mixed; large trials show little effect for most people who aren’t deficient, so don’t take it solely for that.
Take one capsule daily with a meal that contains fat for better absorption. Recheck Vitamin D, 25-Hydroxy and Calcium after 8–12 weeks, then reduce to a maintenance dose once repleted. Thorne D-10,000 is NSF Certified for Sport, which matters if you’re tested. Pairing with magnesium (needed for vitamin D activation) is reasonable if your intake is low. If you routinely need more than 10,000 IU to maintain levels, investigate absorption issues with your clinician rather than escalating indefinitely.
Avoid 10,000 IU without medical supervision if you’ve had high calcium, recurrent kidney stones, sarcoidosis or other granulomatous disease (these can overproduce active vitamin D), or severe kidney disease. Use caution with thiazide diuretics (blood pressure pills that raise calcium) and with digoxin, because high calcium can trigger arrhythmias. Pregnancy and breastfeeding generally use lower daily dosing; only use high-dose under clinician guidance. If you develop nausea, constipation, excessive thirst, or confusion, stop and check Calcium and Vitamin D, 25-Hydroxy promptly.
Frequently asked questions
Is 10,000 IU of vitamin D3 safe to take every day?
It can be safe short term under clinician guidance to correct a low Vitamin D, 25-Hydroxy level. It’s not a lifelong maintenance dose for most adults. Monitor Calcium and Vitamin D, 25-Hydroxy after 8–12 weeks and step down once you’re repleted.
How long does vitamin D3 10,000 IU take to raise my levels?
Most people see a meaningful rise in Vitamin D, 25-Hydroxy within 4–12 weeks. The change depends on starting level, body weight, genetics, and absorption. Re-test at 8–12 weeks to confirm the response and adjust to a lower maintenance dose.
Should I take vitamin D3 with food or on an empty stomach?
Take it with a meal that contains fat to improve absorption. If you’re using bile acid binders or orlistat (which block fat absorption), separate vitamin D3 by at least 2–4 hours so it isn’t carried out of the gut.
Do I need vitamin K2 with vitamin D3?
Vitamin K2 helps activate proteins that handle calcium, but it isn’t required to take with D3. If you use K2, avoid it with warfarin unless your prescriber approves. The key with D3 is monitoring Calcium and Vitamin D, 25-Hydroxy during repletion.
What’s the difference between vitamin D2 and D3?
Vitamin D3 (cholecalciferol) raises and maintains Vitamin D, 25-Hydroxy levels better than D2 (ergocalciferol) in most trials. D2 is prescription in some countries, but for over-the-counter use, D3 is generally the more effective form.
Can high-dose vitamin D3 cause side effects?
Yes—too much can raise calcium too high, causing nausea, constipation, excessive thirst, confusion, or heart rhythm problems. That’s why 10,000 IU should be time-limited and monitored with Calcium and Vitamin D, 25-Hydroxy blood tests.
Does vitamin D3 help the immune system?
If you’re deficient, correcting vitamin D can reduce certain infection risks. For people with adequate levels, large randomized trials show little to no benefit for preventing colds or flu. It’s reasonable to optimize levels, not to megadose for immunity.
How to take it & ingredients
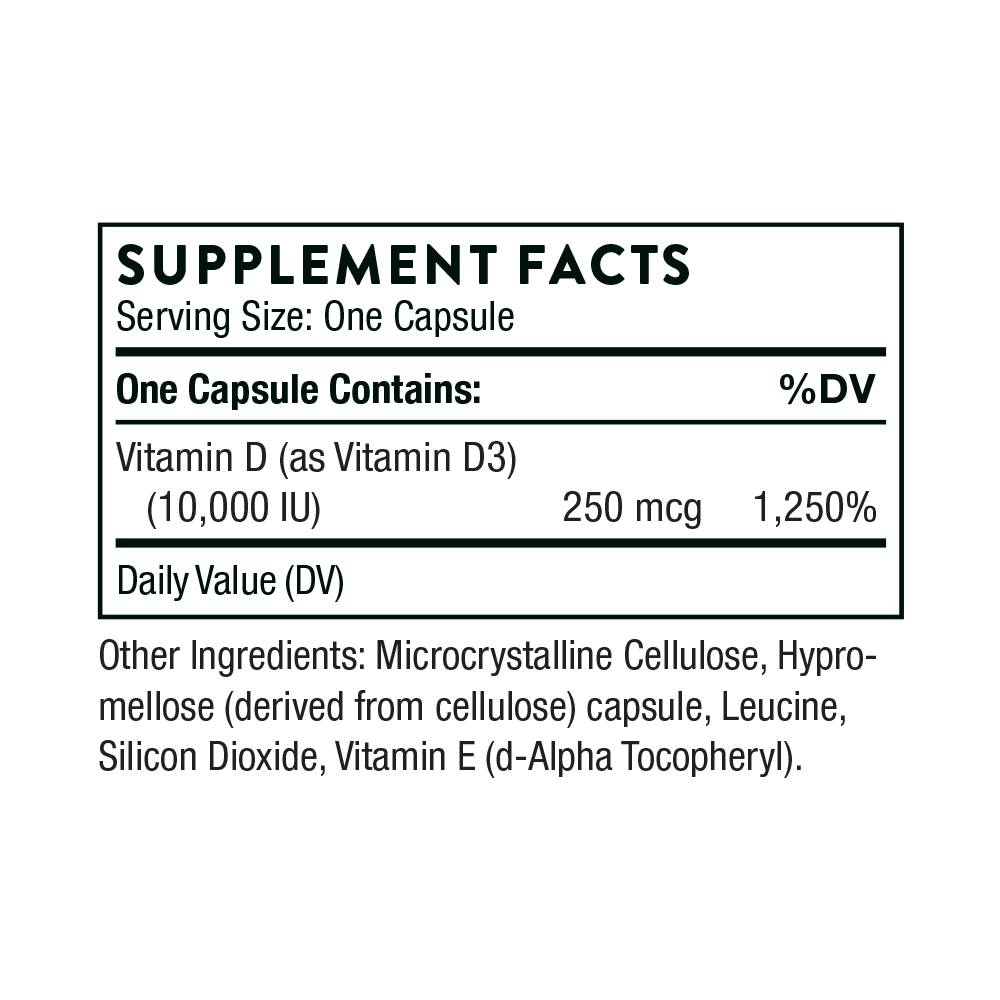
Suggested use: Take 1 capsule daily or as recommended by your health professional.
Active ingredients
1 capsule per serving · 60 servings
Vitamin D
Vitamin D3
Vitamin D3
10000 IU, 250 mcg
Other ingredients: Hypromellose Capsule, Leucine, Microcrystalline Cellulose, Silicon Dioxide, Vitamin E (d-Alpha-Tocopheryl)
Certifications
Benefits
Warnings



