


Klean Athlete
KLEAN-D 1000 IU by Klean Athlete
100 tablets · 100-day supply
Essential Vitamin D for Bone Health and Immune Support$14.00
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Dairy Free
Klean Athlete KLEAN-D 1000 IU overview
If your Vitamin D, 25-Hydroxy is in the lower end of normal and you want a maintenance dose, vitamin D3 1000 IU fits. It suits adults with little midday sun, darker skin, consistent sunscreen use, northern latitudes, or mostly indoor training. The dose is often enough for upkeep in spring and summer. Higher body weight, established deficiency, fat malabsorption, or winter at high latitudes usually require more under clinician guidance, then stepping down to this level.
Cholecalciferol (vitamin D3) is the form your skin makes from sunlight, and it raises blood levels more reliably than D2 (ergocalciferol). Your liver and kidneys convert it into the active hormone that increases calcium absorption from the gut and helps regulate bone turnover. Adequate D3 keeps parathyroid hormone (the signal that pulls calcium from bone) in check. It also supports muscle function and balance. Hopes that vitamin D prevents infections haven’t held up well in controlled trials, so don’t take it for that alone.
Take one tablet daily with a meal that contains some fat, which improves absorption. Morning or evening is fine—consistency matters more than timing. If you’re adjusting dose based on labs, recheck Vitamin D, 25-Hydroxy after 8 to 12 weeks. If you need more than 1,000 IU for repletion, a higher-strength D3 under clinician direction is more practical, then shift back to this for maintenance.
Skip unsupervised vitamin D3 if you have high blood calcium, recurrent calcium kidney stones, or granulomatous diseases like sarcoidosis, which can raise active vitamin D. Thiazide diuretics (blood pressure drugs that reduce calcium loss) increase the risk of high calcium with D3. Orlistat and cholestyramine reduce absorption, while long-term steroids and certain seizure medicines increase vitamin D needs. If you’re pregnant, use vitamin D but set the dose with your clinician and monitor Vitamin D, 25-Hydroxy.
Frequently asked questions
Is 1000 IU of vitamin D3 enough for adults?
It’s a common maintenance dose if your Vitamin D, 25-Hydroxy is low-normal and you get some sun. For established deficiency or higher body weight, most people need a higher short-term repletion dose, then step down to 1,000 IU. Recheck labs in 8–12 weeks.
How long does vitamin D3 1000 IU take to raise levels?
Expect a gradual rise over 8 to 12 weeks. The change depends on your baseline level, body weight, sun exposure, and absorption. If the increase is modest, your clinician may recommend a higher dose temporarily and then return to 1,000 IU.
Should I take vitamin D3 with food or on an empty stomach?
Take it with a meal that includes fat to improve absorption. Taking it on an empty stomach lowers uptake. Time of day is flexible, so pick a predictable meal you rarely miss.
Can I take vitamin D3 with calcium or magnesium?
Yes, vitamin D3 and calcium or magnesium can be taken together. Vitamin D helps absorb calcium. If you have a history of high calcium or kidney stones, involve your clinician and monitor serum calcium along with Vitamin D, 25-Hydroxy.
Does vitamin D3 cause sleep issues if taken at night?
Most people tolerate evening dosing without sleep problems. If you notice lighter sleep or vivid dreams, switch to morning with breakfast. Consistent daily dosing matters more than timing.
What are signs I’m taking too much vitamin D3?
Too much can raise calcium, leading to nausea, constipation, thirst, or frequent urination. This is uncommon at 1,000 IU but possible with higher doses. If you’re escalating dose, monitor Vitamin D, 25-Hydroxy and serum calcium.
Is vitamin D3 safe with blood pressure medicines like thiazides?
Use caution with thiazide diuretics, which reduce calcium loss and can raise calcium when combined with vitamin D. If you’re on thiazides, use a conservative dose and have calcium monitored.
Should athletes take vitamin D3?
Indoor or winter athletes often run low, and normalizing Vitamin D, 25-Hydroxy supports bone health and muscle function. Start with 1,000 IU if you’re low-normal; if your level is low, use a higher, time-limited dose under guidance. Klean Athlete makes this 1,000 IU tablet.
How to take it & ingredients
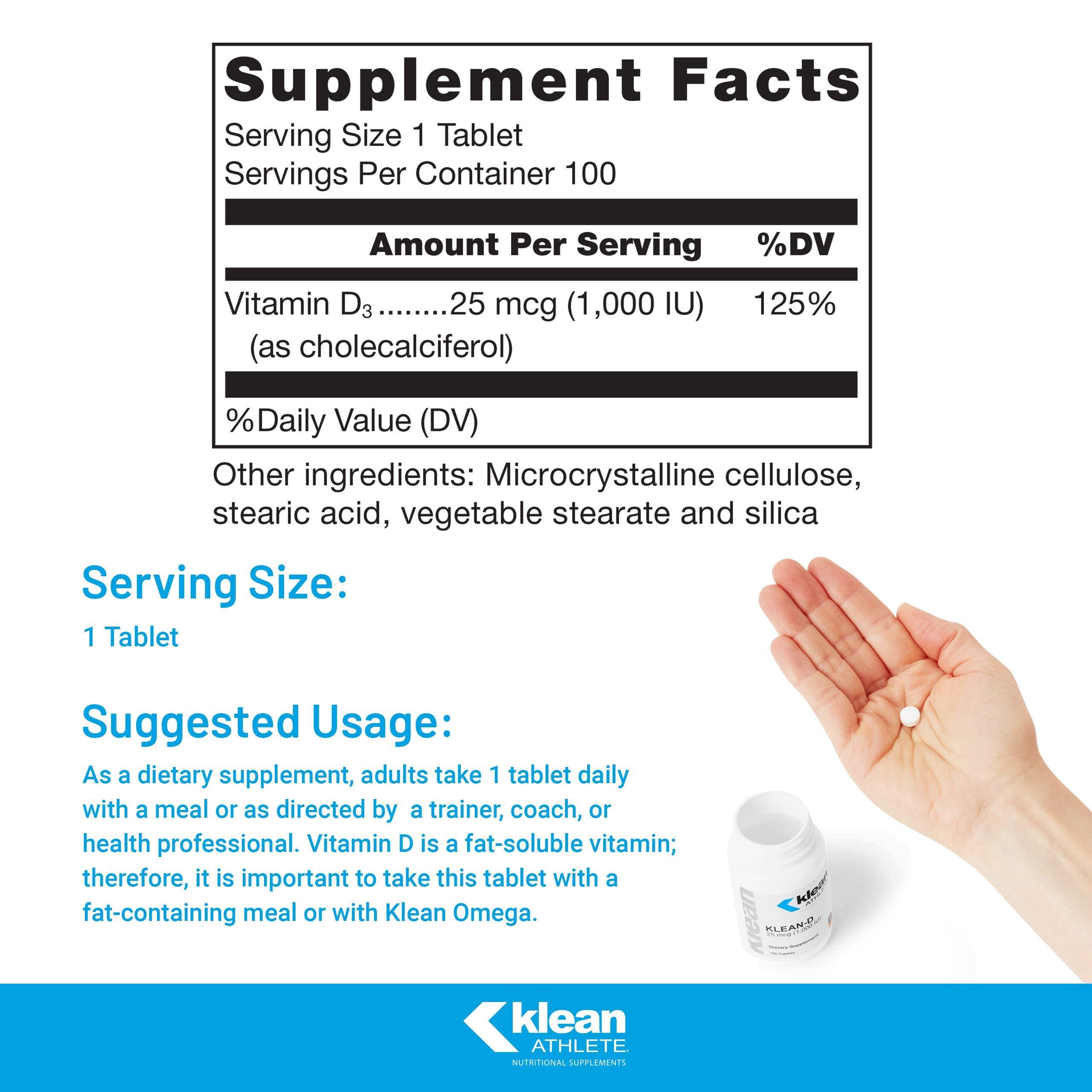
Suggested use: Adults take one (1) tablet daily with a meal or as directed by a trainer, coach, or health professional.
Active ingredients
1 tablet per serving · 100 servings
Vitamin D3
As Cholecalciferol
As Cholecalciferol
1000 IU, 25 mcg
Other ingredients: Microcrystalline cellulose, Vegetable stearate, Silica
Certifications
Benefits
Warnings



