

Dr. Mercola
Vitamins D3 & K2 by Dr. Mercola
30 capsules · 30-day supply
Essential Vitamins for Bone Health and Cardiovascular Support$37.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free
Dr. Mercola Vitamins D3 & K2 overview
Vitamin D3 and K2 suits adults whose Vitamin D, 25-Hydroxy is low or low-normal, especially if you get little sun, have darker skin, live at northern latitudes, or use sunscreen consistently. The 5,000 IU D3 here is a repletion-leaning daily dose for many, useful if your level hasn’t budged with 1,000–2,000 IU. K2 (MK-7) matters if you take calcium or have bone density concerns, because it helps steer calcium into bone. Higher body weight often requires more D3 to reach the same blood level; confirm with labs after 8–12 weeks.
Cholecalciferol (vitamin D3) is the form your skin makes from sunlight, and it raises Vitamin D, 25-Hydroxy more reliably than D2. As D3 rises, it increases calcium absorption and helps quiet parathyroid hormone (the signal that pulls calcium from bone). Vitamin K2 as MK-7 activates proteins like osteocalcin in bone and matrix Gla protein in arteries, which guide calcium into skeleton and keep it out of soft tissues. MK-7 has a longer half-life than K1 or MK-4, so a once-daily dose maintains steadier activation. D3 for infections was overhyped; large trials haven’t shown clear prevention.
Take one capsule daily with a meal that contains fat for better absorption. Recheck Vitamin D, 25-Hydroxy after 8–12 weeks to see if 5,000 IU is enough, then adjust. If your level is significantly low, short-term higher dosing under clinician guidance is common, then step down. You can take vitamin D3 and K2 any time of day; consistency beats timing. Pairing with magnesium is reasonable, since magnesium is a cofactor for vitamin D metabolism.
If you take warfarin (a vitamin K–antagonist blood thinner), skip vitamin K2 unless your prescriber plans frequent INR checks and dose adjustments. Other direct oral anticoagulants aren’t vitamin K–dependent but still warrant a quick check-in. Very high vitamin A plus high-dose D3 can raise calcium too much; keep vitamin A moderate. If your Calcium or PTH (parathyroid hormone test) is abnormal, get medical guidance before using higher-dose D3.
Avoid high-dose D3 if you have a history of high calcium, recurrent kidney stones, granulomatous conditions like sarcoidosis, or primary hyperparathyroidism until evaluated. Pregnancy and breastfeeding require individualized dosing; bring your labs to your obstetric clinician. If your Vitamin D, 25-Hydroxy is already high, this strength from Dr. Mercola is likely too much for maintenance—use a lower-dose D3 or take less frequently.
Frequently asked questions
How long does vitamin D3 and K2 take to work?
Most people see Vitamin D, 25-Hydroxy move meaningfully within 4–12 weeks on a steady dose. Bone effects take longer; you’re guiding calcium handling over months. Recheck labs at 8–12 weeks, then every few months until stable.
Should I take vitamin D3 and K2 with food or on an empty stomach?
With food. Both are fat-soluble, so a meal containing fat improves absorption. Taking it the same way each day matters more than the exact time of day.
Is 5,000 IU of vitamin D3 too much to take daily?
It’s a common daily dose for bringing up low levels, but it’s more than a typical maintenance dose. Use it short to medium term, then adjust based on Vitamin D, 25-Hydroxy. If your level is already high, use a lower dose.
Can I take vitamin D3 and K2 with calcium and magnesium?
Yes. D3 improves calcium absorption, K2 helps direct it to bone, and magnesium supports vitamin D metabolism. If you take separate calcium, keep the total daily amount reasonable to avoid excess.
Does vitamin D3 and K2 thin your blood?
No. Vitamin K2 affects calcium-handling proteins, not thinning. However, vitamin K can counteract warfarin. If you’re on warfarin, do not start K2 without prescriber oversight and INR monitoring.
What’s the difference between K2 MK-7 and MK-4?
MK-7 stays in the bloodstream longer and maintains steadier activation of vitamin K–dependent proteins with once-daily dosing. MK-4 has a shorter half-life and typically needs multiple daily doses.
Is vitamin D3 better than D2?
Yes for most people. D3 (cholecalciferol) raises and maintains Vitamin D, 25-Hydroxy more effectively than D2 (ergocalciferol). If you’re vegan, algae-derived D3 is an option.
How to take it & ingredients
Suggested use: Adults take one capsule daily, with food, or as directed by your healthcare professional.
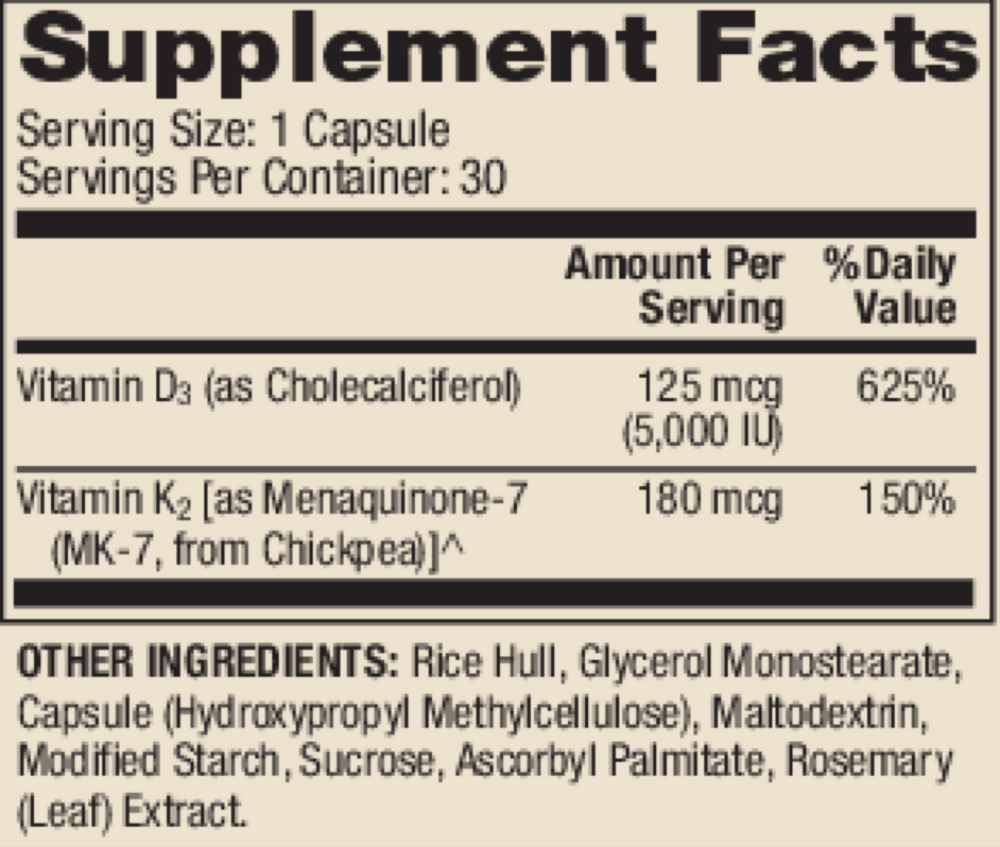
Active ingredients
1 capsule per serving · 30 servings
Vitamin D
Cholecalciferol
Cholecalciferol
125 mcg, 5000 IU
Vitamin K
Vitamin K2 (Menaquinone-7 [MK-7], from Chickpea)
Vitamin K2 (Menaquinone-7 [MK-7], from Chickpea)
180 mcg
Other ingredients: Hydroxypropyl Methylcellulose Capsule, Microcrystalline Cellulose, Calcium Laurate, Silicon Dioxide
Certifications
Benefits
Warnings
Customers also considered

Ortho Molecular Products
K-FORCE
60 capsules
$60.33extra 10% off with Subscribe & Save

Ortho Molecular Products
K-FORCE MAX
30 capsules
$44.79extra 10% off with Subscribe & Save

Ortho Molecular Products
Liquid Vitamin D3 with K2
30 milliliters
$52.00extra 10% off with Subscribe & Save

NBI
Osteo-K Minis
120 capsules
$65.99extra 20% off with Subscribe & Save