

Garden of Life
Vitamin Code Raw D3 5000 IU by Garden of Life
60 capsules · 60-day supply
Essential Vitamin D3 for Bone, Immune, and Mood Support$29.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Vegetarian·Kosher·Gluten Free·Preservative Free·Artificial Color Free·
Garden of Life Vitamin Code Raw D3 5000 IU overview
If your Vitamin D, 25-Hydroxy is low or in the lower part of the normal range, vitamin D3 5000 IU is a practical repletion step. It’s a fit for darker‑skinned adults, indoor workers, northern latitudes, consistent sunscreen users, older adults, people with higher body weight, and those with fat malabsorption or after bariatric surgery. If your level is already solid, this dose can overshoot; consider a lower maintenance vitamin D3 and re‑test to guide.
Cholecalciferol (vitamin D3) is the form your skin makes from sunlight, and it raises blood levels more reliably than D2. Your liver and kidneys convert it into the active hormone that increases calcium absorption from the gut and helps regulate bone remodeling. Adequate vitamin D3 tames parathyroid hormone (the signal that pulls calcium from bone). The added probiotic/enzyme and fruit‑vegetable blends are fine, but evidence that they change vitamin D absorption or outcomes is limited.
Take one capsule daily with food that contains fat, since vitamin D3 is fat‑soluble and absorbs better with a meal. Recheck Vitamin D, 25-Hydroxy in 8–12 weeks to see if you’ve reached your target zone, then adjust to a maintenance dose. Morning or evening is fine. If you routinely need more than 1000–2000 IU for upkeep after repletion, stick with a higher‑dose capsule for practicality.
Avoid vitamin D3 5000 IU if you’ve had high calcium, recurrent kidney stones, sarcoidosis or other granulomatous diseases (they can raise active vitamin D internally), or primary hyperparathyroidism. Use caution if you take thiazide diuretics (blood‑pressure meds that can raise calcium) or digoxin. Orlistat and bile‑acid binders cut absorption; separate dosing by several hours. Pregnancy or breastfeeding: use only with clinician guidance and lab follow‑up.
Frequently asked questions
How long does it take vitamin D3 5000 IU to raise my levels?
Most people see meaningful changes in Vitamin D, 25-Hydroxy within 8–12 weeks. The shift depends on baseline level, body weight, sun exposure, and consistency. Re-test at that point and adjust to a maintenance dose once you’re where you want to be.
Is vitamin D3 5000 IU safe to take every day?
It’s commonly used short term to correct low levels, with labs guiding duration. Long‑term daily use can overshoot in people who don’t need it. Signs of excess relate to high calcium (thirst, frequent urination, constipation). Periodic blood tests keep it safe.
Do I need vitamin K2 with vitamin D3?
Not necessarily. Vitamin K2 helps activate proteins that handle calcium, but adding K2 hasn’t consistently changed fracture or heart outcomes in trials. If your diet is low in K‑rich foods, K2 may be reasonable, yet it isn’t required to take vitamin D3 safely.
Should I take vitamin D3 in the morning or at night?
Either works. Consistency and taking it with a meal that contains fat matter more than time of day. Some people prefer morning to avoid the chance of sleep disruption, though most do not notice an effect on sleep.
Which medications interact with vitamin D3?
Thiazide diuretics can raise calcium, so combining with high‑dose D3 raises hypercalcemia risk. Orlistat and bile‑acid binders reduce absorption; separate by several hours. Chronic steroids and some anti‑seizure drugs lower vitamin D, often requiring higher monitored dosing.
Can vitamin D3 cause kidney stones?
High vitamin D can raise calcium, which may raise stone risk in susceptible people. If you have a history of calcium stones, use vitamin D3 under clinician guidance with periodic checks of calcium and Vitamin D, 25-Hydroxy, and emphasize hydration.
Does vitamin D3 thin your blood?
No. Vitamin D3 is not a blood thinner and does not replace anticoagulants. If you’re on warfarin or other blood thinners, vitamin D3 is generally compatible, but always coordinate supplements with your prescribing clinician.
Do I need magnesium with vitamin D3?
Magnesium is a cofactor for vitamin D metabolism. If your intake is low, correcting magnesium can help vitamin D work properly. You don’t have to take them together, but ensuring adequate magnesium from diet or supplements is sensible.
How to take it & ingredients
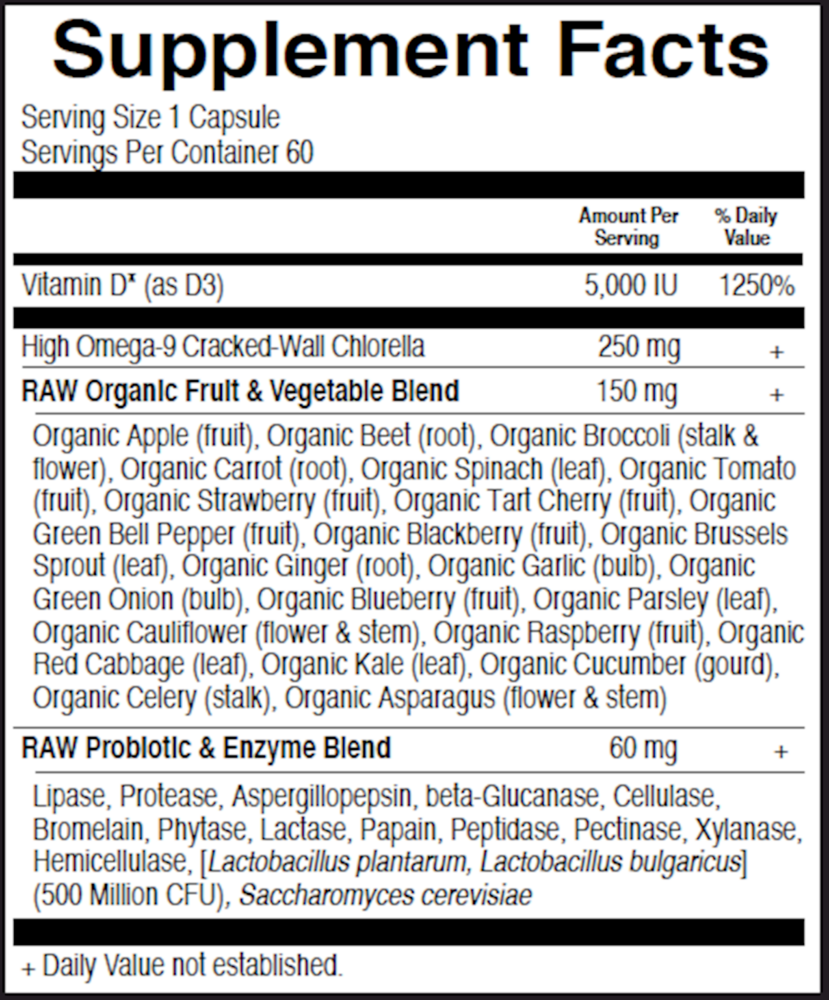
Suggested use: Adults take 1 capsule daily. Best taken with food.
Active ingredients
1 capsule per serving · 60 servings
Vitamin D
Vitamin D3
Vitamin D3
5000 IU, 125 mcg
RAW Food, Probiotic & Enzyme Blend
285 mg
RAW Organic Fruit & Vegetable Blend
150 mg
Other ingredients: Vegetable cellulose, Brewers Yeast (Saccharomyces cetevisiae), Lactobacillus bulgaricus
Certifications
Benefits
Warnings



