
Garden of Life
VitaminCode Healthy Blood by Garden of Life
60 capsules · 30-day supply
Comprehensive Nutrients for Healthy Blood and Vitality Support$18.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Vegetarian·Gluten Free·Dairy Free·Preservative Free
Garden of Life VitaminCode Healthy Blood overview
If your Ferritin (the storage form of iron) is low or your Hemoglobin (oxygen-carrying protein on a blood count) runs low, an iron supplement like this is a practical repletion dose. It suits heavy menstrual bleeders, vegans and vegetarians, frequent blood donors, endurance athletes, and people after surgery. It’s also a fit when B12 or folate are borderline on labs, since those vitamins drive red blood cell production. If your levels are severely low, you may need a clinician-guided plan first, then use this for ongoing repletion.
Iron is the core mineral your bone marrow uses to build hemoglobin, and vitamin C improves its absorption from the gut. Folate and vitamin B12 enable DNA steps needed to make new red blood cells, while vitamin B6 helps hemoglobin assembly. Together, they raise Hemoglobin and refill Ferritin over weeks, not days. The probiotic and enzyme blend aims to improve tolerance; some patients report fewer stomach issues, though the clinical evidence for probiotics reducing iron side effects is limited.
The label calls for two capsules daily, with or without food. Iron absorbs best on an empty stomach with water or vitamin C, but if you feel nauseated, take it with a small meal. Avoid taking it within two hours of coffee, tea, dairy, calcium, or fiber supplements because they block absorption. Expect energy and exercise tolerance to improve within 4 to 8 weeks if low iron was the cause, and plan to recheck Ferritin and Hemoglobin at 8 to 12 weeks.
Separate iron by at least four hours from levothyroxine (thyroid hormone) and from antibiotics like doxycycline and fluoroquinolones, since iron binds them and reduces their effect. Antacids and acid reducers can lower iron uptake; space dosing by two to four hours. Vitamin C enhances absorption, while calcium, zinc, and magnesium compete. If you take a multivitamin, don’t double up on iron unless a clinician has reviewed your labs.
Skip iron if your Ferritin is high, you have hemochromatosis (a genetic iron overload), chronic liver disease with high iron stores, or repeated transfusions. Active inflammatory bowel flares or untreated celiac can make oral iron intolerable—get guidance. Black stools are common with iron, but tarry stools with weakness or dizziness deserve urgent care. Keep all iron away from children; accidental overdose is a medical emergency.
Frequently asked questions
How long does it take for iron supplements to raise ferritin?
Most people see ferritin rise within 8–12 weeks, but full repletion can take several months depending on how low you started and ongoing losses like heavy periods. Recheck Ferritin and Hemoglobin at 8–12 weeks to gauge progress and adjust.
Is 28 mg of iron a lot?
It’s a typical therapeutic daily dose for iron deficiency in adults. It’s higher than standard dietary intake and is intended for repletion, not casual use. Confirm low Ferritin or anemia with labs before starting and avoid doubling up with other iron sources.
Can iron supplements cause constipation or nausea?
Yes. Constipation, dark stools, nausea, and abdominal discomfort are common. Taking iron with a small meal, hydrating, adding fiber, or splitting the dose can help. If symptoms are severe or persistent, talk to your clinician about alternate forms or dosing.
Can I take iron with coffee or dairy?
Avoid coffee, tea, and dairy within two hours of iron. Compounds in coffee and tea (polyphenols) and calcium in dairy reduce iron absorption. Water or vitamin C–containing beverages are better choices when you take your dose.
Can I take iron if I’m on thyroid medication?
Yes, but separate doses. Iron binds levothyroxine and can blunt its absorption. Take levothyroxine on an empty stomach, then wait at least four hours before taking your iron supplement to avoid interference.
Do men need iron supplements?
Usually not unless labs show low Ferritin or anemia and a cause is identified. Men lack monthly iron losses, so unexplained low iron warrants evaluation for bleeding or absorption issues before starting supplementation.
Is this iron supplement safe in pregnancy?
Iron needs rise in pregnancy, but dosing should follow prenatal labs. Many patients use 27–30 mg daily when iron is low; confirm with your obstetric clinician and monitor Hemoglobin and Ferritin during pregnancy.
What’s the difference between heme and non-heme iron?
Heme iron (from animal foods) absorbs more efficiently, while most supplements provide non-heme iron, which absorbs well with vitamin C. Both can replete low stores; absorption hinges on timing, co-ingestion, and your baseline iron status.
How to take it & ingredients
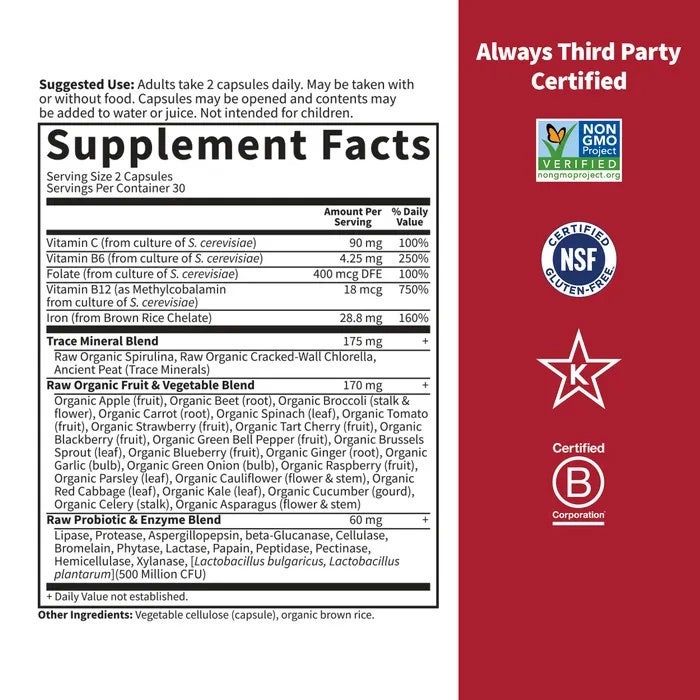
Suggested use: Adults take 2 capsules daily. May be taken with or without food.
Active ingredients
2 capsules per serving · 30 servings
Vitamin C
60 mg
Vitamin B6
5 mg
Folate
400 mcg
Vitamin B12
45 mcg
Iron
28 mg
RAW Veggie Mineral Blend
200 mg
RAW Food Probiotic & Enzyme Blend
75 mg
Other ingredients: Vegetable cellulose, Brewers yeast (Saccharomyces cerevisiae), Lactobacillus bulgaricus
Certifications
Benefits
Warnings
Customers also considered

Thorne
Iron Bisglycinate
60 capsules
$16.00extra 10% off with Subscribe & Save

Now Foods
Iron Complex
100 tablets
$13.99extra 21% off with Subscribe & Save

Life Extension
Iron Protein Plus 300 mg
100 capsules
$28.99extra 21% off with Subscribe & Save

Ortho Molecular Products
Reacted Iron
60 capsules
$29.58extra 10% off with Subscribe & Save