

Ortho Molecular Products
Reacted Iron 29 mg by Ortho Molecular Products
60 capsules · 60-day supply
Gentle Iron Support for Healthy Blood and Energy Levels$29.58
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Reacted Iron overview
Heavy periods with low Ferritin or a dipping Hemoglobin on a CBC is the classic scenario where iron bisglycinate shines. It also fits frequent blood donors, pregnancy planning or second/third trimester under clinician care, vegans on restrictive diets, endurance athletes, and post-bariatric surgery patients. If Proton Pump Inhibitors (acid-blockers) or celiac reduce absorption, this gentler form often works when ferrous sulfate doesn’t. The 29 mg here is a practical daily dose for maintenance or mild deficiency; established anemia usually needs a higher or clinician-directed schedule.
Ferrous bisglycinate is iron bound to two glycine molecules, which helps it pass through the gut with fewer reactions to food and less irritation than ferrous sulfate. Once absorbed, iron rebuilds hemoglobin (the oxygen carrier in red blood cells) and myoglobin in muscle, and feeds mitochondrial enzymes that make ATP, your cell’s energy currency. Hepcidin (a liver hormone that gates iron absorption) rises with inflammation and with too-frequent dosing, which is why this form and smart scheduling improve uptake and tolerability.
Take one capsule daily, ideally away from calcium-rich foods, coffee, or tea, which block absorption. A small snack is fine if empty-stomach iron upsets you. Vitamin C (a glass of citrus or 250–500 mg) can improve uptake. Some clinicians use every-other-day dosing to work with hepcidin and reduce nausea. Expect Hemoglobin to start rising within 2–4 weeks and Ferritin to climb over 4–12 weeks, then continue several months to refill iron stores.
Skip iron unless advised if you have hemochromatosis, thalassemia, repeated transfusions, or active infection. Separate by at least 2 hours from levothyroxine, zinc or magnesium supplements, and by 4 hours from tetracycline or fluoroquinolone antibiotics and oral bisphosphonates; iron blocks their absorption. Long-term use of Proton Pump Inhibitors can blunt iron uptake—monitor Ferritin, Hemoglobin, and Transferrin Saturation to be sure you’re responding.
Frequently asked questions
Is iron bisglycinate easier on the stomach than ferrous sulfate?
Yes. The bisglycinate chelate is typically better tolerated with less nausea and constipation than ferrous sulfate. It also interacts less with food inhibitors, which can improve absorption if you can’t take iron on an empty stomach.
How long does it take iron to raise ferritin and hemoglobin?
Hemoglobin usually improves within 2–4 weeks if you’re absorbing it, while Ferritin (your iron stores) rises over 4–12 weeks. Continue for several months after symptoms improve to replete stores, guided by repeat labs.
Can I take iron with coffee, tea, or dairy?
It’s best to avoid them around your dose. Coffee, tea, and calcium-rich foods reduce iron absorption. Leave a 1–2 hour window away from those, and consider pairing iron with vitamin C to improve uptake.
Does iron cause constipation, and what can help?
Constipation can occur with any iron, but bisglycinate causes it less often. Hydration, magnesium glycinate at night, fiber, and every-other-day dosing can help. If symptoms persist, check with your clinician and confirm you’re responding on labs.
Can men take iron bisglycinate?
Only if labs confirm low iron. Adult men rarely need supplemental iron and can accumulate excess. If your Ferritin or Transferrin Saturation is low, use iron short term under clinician supervision with repeat testing.
Is iron bisglycinate safe in pregnancy?
Often, yes, and it’s commonly chosen for better tolerance. Dosing in pregnancy should be clinician-directed with monitoring of Hemoglobin and Ferritin. Do not start iron in pregnancy based on symptoms alone.
Can I take iron with levothyroxine or antibiotics?
Separate them. Take levothyroxine at least 2 hours apart from iron. For tetracycline or fluoroquinolone antibiotics and oral bisphosphonates, separate by 4 hours to prevent reduced drug absorption.
Is every-other-day iron as effective as daily?
For many people, yes. Spacing doses can lower hepcidin and improve absorption while reducing side effects. If you use this approach, confirm progress with Hemoglobin and Ferritin after 4–8 weeks.
How to take it & ingredients
Suggested use: Take 1 capsule per day or as recommended by your health care professional.
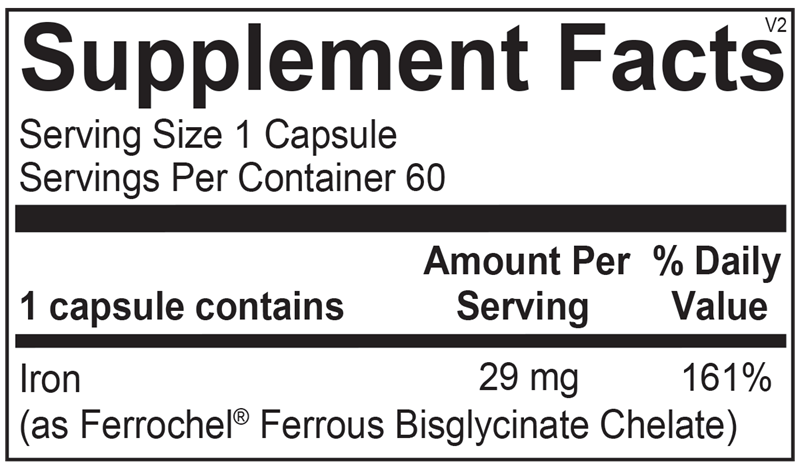
Active ingredients
1 capsule per serving · 60 servings
Iron
Ferrochel® Ferrous Bisglycinate Chelate
Ferrochel® Ferrous Bisglycinate Chelate
29 mg
Other ingredients: Microcrystalline Cellulose, Hypromellose (Natural Vegetable Capsule), Magnesium Stearate
Certifications
Benefits
Warnings
Customers also considered

Thorne
Iron Bisglycinate
60 capsules
$16.00extra 10% off with Subscribe & Save

Now Foods
Iron Complex
100 tablets
$13.99extra 21% off with Subscribe & Save

Life Extension
Iron Protein Plus 300 mg
100 capsules
$28.99extra 21% off with Subscribe & Save
Garden of Life
VitaminCode Healthy Blood
60 capsules
$18.99extra 21% off with Subscribe & Save