


Now Foods
Iron Complex by Now Foods
100 tablets · 100-day supply
Comprehensive Iron Support with Essential Vitamins and Botanicals$13.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Vegetarian·Halal Certified·Kosher·Gluten Free·Soy Free·
Now Foods Iron Complex overview
If your Ferritin (the protein that stores iron) or Hemoglobin (the oxygen-carrying protein in red blood cells) is low, iron bisglycinate is a gentle way to replete without the usual constipation. It fits heavy menstrual bleeders, vegetarians and vegans, postpartum adults, frequent blood donors, endurance athletes, and anyone with low energy tied to iron labs. If your deficiency is significant or ongoing blood loss continues, you’ll likely need higher-dose iron or clinician-guided therapy first, then step down to this daily maintenance.
Ferrochel iron bisglycinate is iron bound to two glycine amino acids, which protects it from binding to food and makes it easier on the gut. The 27 mg dose feeds hemoglobin building to improve oxygen delivery, while vitamin C increases iron absorption in the small intestine. Folate and vitamin B12 support red cell formation alongside iron. The botanicals (dong quai and red raspberry leaf) are included for menstrual comfort, though their effects are milder and not a substitute for correcting low iron stores.
Take one tablet daily with a meal as NOW suggests. Absorption is highest away from calcium, coffee, tea, and high‑fiber bran, so pick a meal without those. Many clinicians prefer morning or mid‑afternoon. If your stomach is sensitive, food is fine, and this form stays gentle. Recheck Ferritin and Hemoglobin within 8 to 12 weeks; energy often improves sooner, while iron stores usually take a few months to rebuild. For established deficiency, alternate‑day higher dosing may be advised by your clinician.
Avoid iron if you have iron overload conditions like hemochromatosis, repeated transfusions, or thalassemia, or if your Ferritin is already high. Dong quai can increase bleeding risk, so skip if you use blood thinners like warfarin, apixaban, or rivaroxaban, or if you have hormone‑sensitive cancers. Pregnancy: avoid dong quai; ask your obstetric clinician before use. Iron binds certain meds—separate by several hours from levothyroxine, doxycycline, tetracyclines, fluoroquinolones, and osteoporosis drugs.
Frequently asked questions
How long does iron bisglycinate take to raise ferritin?
Most people see ferritin rise within 8–12 weeks, but fully rebuilding iron stores can take 3–6 months depending on the cause of loss. Energy may improve sooner as hemoglobin recovers. Retest Ferritin and Hemoglobin to track progress and continue several months after levels normalize.
Is iron bisglycinate less constipating than ferrous sulfate?
Yes. Iron bisglycinate is typically gentler on the stomach with less constipation and nausea than ferrous sulfate at similar elemental iron doses. If you still get constipated, hydrate, add magnesium or fiber, or try alternate‑day dosing after speaking with your clinician.
Can I take iron with coffee or calcium?
It’s better not to. Coffee, tea, and calcium compete with iron absorption. Take iron bisglycinate with water and a meal that doesn’t include dairy or calcium supplements, and wait a couple of hours before or after coffee or tea for best uptake.
Does iron interact with levothyroxine or antibiotics?
Yes. Iron binds levothyroxine and several antibiotics, reducing absorption of both. Separate iron by at least 4 hours from levothyroxine, doxycycline, tetracyclines, fluoroquinolones, and osteoporosis drugs like alendronate. Ask your pharmacist if you’re unsure about timing.
Is the B12 form (cyanocobalamin) okay if I prefer methylcobalamin?
Cyanocobalamin is well‑studied, stable, and effective for most people. If you have a true cobalamin deficiency or specific preferences, methylcobalamin is a reasonable alternative. What matters most is rechecking B12 and methylmalonic acid if deficiency is suspected.
Can iron bisglycinate help with heavy periods or fatigue?
If fatigue is driven by low Hemoglobin or Ferritin from heavy menstrual bleeding, repleting iron often helps within weeks. The included dong quai and raspberry leaf are for menstrual comfort but won’t correct low iron on their own; labs guide whether iron is the right lever.
Is iron safe in pregnancy or breastfeeding?
Iron can be appropriate in pregnancy if labs show low stores, but dong quai is generally avoided. Use a plain prenatal iron or consult your obstetric clinician before using this formula. During breastfeeding, confirm need with labs and your clinician.
Do acid‑reducing drugs affect iron absorption?
Yes. Proton pump inhibitors (acid‑reducing drugs like omeprazole) and H2 blockers lower stomach acid and can reduce iron uptake. Using vitamin C with iron helps, but you may need lab‑guided dosing or a clinician’s input if you’re on these medications.
How to take it & ingredients
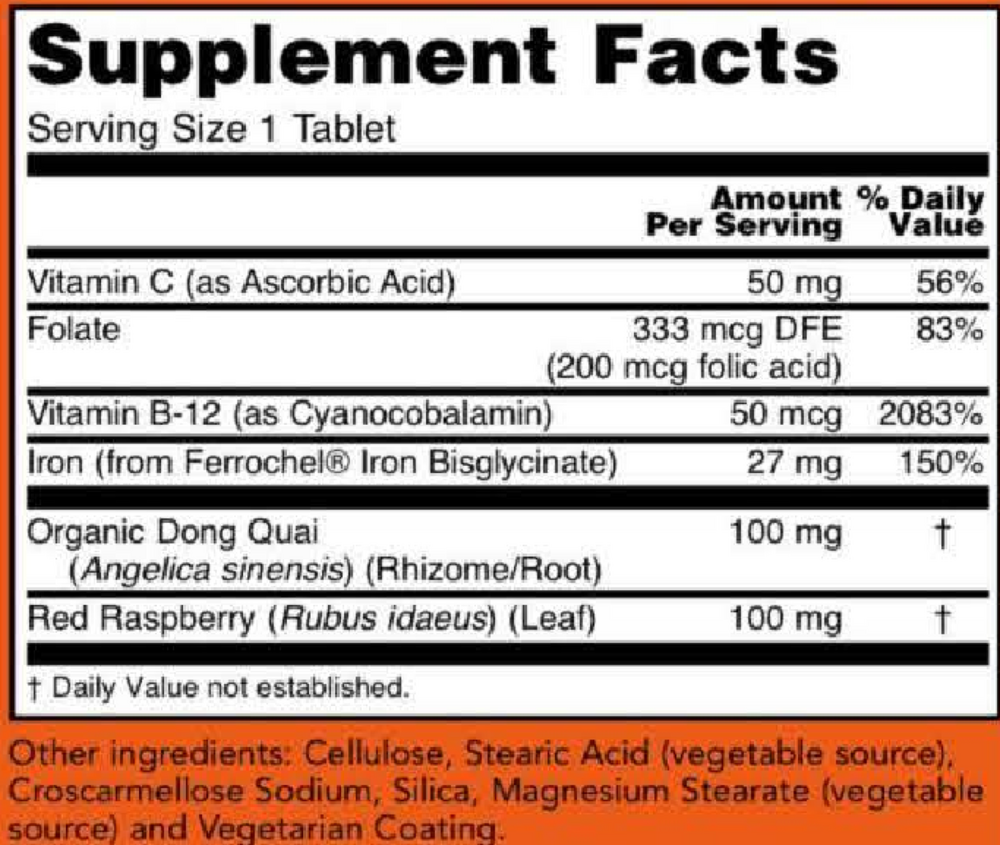
Suggested use: Take 1 tablet daily with a meal.
Active ingredients
1 tablet per serving · 100 servings
Vitamin C
Ascorbic acid
Ascorbic acid
50 mg
Folate
Folic acid
Folic acid
333 mcg DFE, 200 mcg
Vitamin B12
Cyanocobalamin
Cyanocobalamin
50 mcg
Iron
Ferrochel iron bisglycinate
Ferrochel iron bisglycinate
27 mg
Dong Quai
Angelica sinensis (rhizome/root)
Angelica sinensis (rhizome/root)
100 mg
Red Raspberry
Rubus idaeus (leaf)
Rubus idaeus (leaf)
100 mg
Other ingredients: Cellulose, Stearic acid (vegetable source), Croscarmellose sodium, Silica, Magnesium stearate (vegetable source), Vegetarian coating
Certifications
Benefits
Warnings
Customers also considered

Thorne
Iron Bisglycinate
60 capsules
$16.00extra 10% off with Subscribe & Save

Life Extension
Iron Protein Plus 300 mg
100 capsules
$28.99extra 21% off with Subscribe & Save

Ortho Molecular Products
Reacted Iron
60 capsules
$29.58extra 10% off with Subscribe & Save
Garden of Life
VitaminCode Healthy Blood
60 capsules
$18.99extra 21% off with Subscribe & Save