




Klean Athlete
Klean Omega 1250 mg by Klean Athlete
60 softgels · 60-day supply
Premium Fish Oil for Heart, Brain, and Joint Health$44.50
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Egg Free·Tree Nut Free·Peanut Free·Wheat Free·
Klean Athlete Klean Omega overview
If you train hard and eat little seafood, fish oil for athletes is a simple way to raise EPA and DHA, the omega-3 fats that show up on the Omega-3 Index. This one-softgel routine suits maintenance: keeping levels steady, smoothing post‑training soreness, and nudging hs-CRP (a blood marker of inflammation) down in some responders. If your triglycerides are elevated or your Omega-3 Index is low, you will likely need a higher EPA+DHA dose than a single softgel provides.
EPA and DHA reduce how much fat your liver sends out in VLDL particles (the form that shows up as triglycerides on a lipid panel), and they push cells to burn fats for energy more readily. Within 4 to 12 weeks, many people see triglycerides drop 20–30% at clinical doses. These fats also shift cell-membrane signaling toward fewer pro‑inflammatory eicosanoids (short‑lived chemical messengers), which tracks with modest hs-CRP reductions in some athletes.
Take one softgel with a meal that contains fat to improve absorption and reduce fishy aftertaste. Consistency matters more than time of day. If your goal is triglyceride reduction, typical effective intakes are higher EPA+DHA totals than maintenance products provide, so consider a concentrate with known EPA and DHA amounts and recheck your Omega-3 Index and triglycerides after 8 to 12 weeks.
Pause fish oil before surgery and use caution if you take blood thinners like warfarin, apixaban, clopidogrel, or high‑dose aspirin, since bleeding risk can rise slightly. If you have a fish or shellfish allergy, choose an algae-based DHA/EPA. Some people see a small LDL cholesterol bump, especially with DHA‑heavy oils, so pair use with a lipid panel. Pregnancy needs DHA, but pick a product with stated DHA per softgel.
Krill oil is fine but usually delivers less EPA+DHA per capsule, so cost per gram is higher. Burp control tips: take with your largest meal, keep capsules in the freezer, or use enteric‑coated fish oil. If you are vegetarian or vegan, algae oil provides preformed DHA and often some EPA, and it reliably moves the Omega-3 Index.
Frequently asked questions
How long does fish oil take to lower triglycerides?
At clinical EPA+DHA intakes, changes appear within 4 to 12 weeks. Recheck a lipid panel after 8 to 12 weeks. A single maintenance softgel is usually too low for triglyceride reduction; look for products listing total EPA+DHA in grams.
Does fish oil thin your blood?
It has a mild anti‑platelet effect, which can slightly increase bleeding risk. Most healthy people are fine, but if you take warfarin, apixaban, clopidogrel, or high‑dose aspirin, talk to your clinician and pause before surgery.
What’s the best time to take omega-3 fish oil?
Take it with a meal that contains fat to improve absorption and reduce fishy burps. Morning or evening both work. Consistency day to day matters more than timing around workouts.
Can fish oil cause higher LDL cholesterol?
A small LDL increase can occur in some people, more often with DHA‑heavy oils, while triglycerides drop. Track your lipid panel after 8 to 12 weeks and adjust your formula or dose if LDL meaningfully rises.
Is algae oil as effective as fish oil?
For raising the Omega-3 Index and delivering DHA, algae oil works well and suits those avoiding fish. For triglyceride lowering, match the EPA+DHA grams to fish‑oil trials; some algae products are lower per capsule.
How much EPA and DHA do I need daily?
For maintenance, 250–500 mg combined EPA+DHA works for many diets low in fish. For triglyceride reduction, clinical trials use higher amounts per day. Choose a product that lists EPA and DHA per serving so you can match your goal.
Will omega-3 help with workout recovery?
It can modestly reduce next‑day muscle soreness and hs-CRP in some athletes, especially if baseline omega‑3 status is low. Effects build over weeks; it is not an immediate pain reliever.
How to take it & ingredients
Suggested use: As a dietary supplement, adults take 1 softgel daily with a meal or as directed by a healthcare professional.
Active ingredients
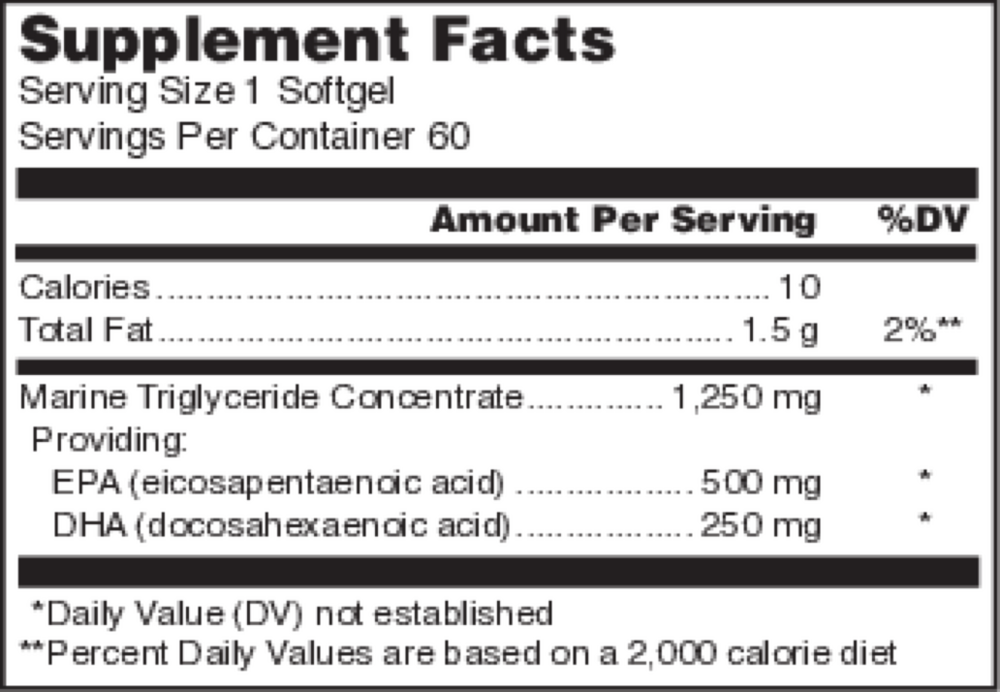
1 softgel per serving · 60 servings
▼
Marine Triglyceride Concentrate
1250 mg
EPA
Eicosapentaenoic acid
Eicosapentaenoic acid
500 mg
DHA
Docosahexaenoic acid
Docosahexaenoic acid
250 mg
Other ingredients: Fish gelatin (capsule, from tilapia), Purified water, Natural orange flavor, Natural mixed tocopherols
Certifications
Benefits
Warnings
Customers also considered

Thorne
Advanced DHA
60 gelcaps
$30.00extra 10% off with Subscribe & Save

Garden of Life
Dr. Formulated Advanced Omega
60 softgels
$31.99extra 19% off with Subscribe & Save
Garden of Life
Dr. Formulated DHA 1g
30 softgels
$31.99extra 19% off with Subscribe & Save
Garden of Life
Dr. Formulated Prenatal DHA
30 softgels
$29.99extra 20% off with Subscribe & Save