

Metagenics
UltraFlora Acute Care Probiotic by Metagenics
30 capsules · 30-day supply
Targeted Probiotic Support for Digestive Health and Balance$XX.XX$43.99retail
This item is currently out of stockGet notified when this item is back in stock
20% below MSRP3rd-party testedFree shipping $50+
Vegetarian·Gluten Free
Metagenics UltraFlora Acute Care Probiotic overview
Travelers and anyone starting antibiotics are the main groups who benefit. Saccharomyces boulardii (a probiotic yeast) reduces antibiotic-associated diarrhea and shortens many cases of acute infectious diarrhea. If your stool testing points to C. difficile toxin or you have loose stools after antibiotics, this is often the right first move. If your Calprotectin (a stool inflammation marker) is high or there is blood, see a clinician before self-treating.
S. boulardii is a live yeast that does not colonize long term but competes with pathogens, binds toxins, and increases secretory IgA (the antibody that lines the gut). It makes enzymes that degrade C. difficile toxins and reduces water loss in the intestine. The companion lactobacillus and bifidobacterium strains help restore a healthy balance after disruption, which is why loose stools often settle within 24 to 72 hours in responders.
Take one capsule once or twice daily at the first sign of loose stools, with or without food, for 5 to 14 days. During antibiotics, separate the dose by at least 2 to 3 hours and continue for a week after the last pill. For prevention during travel, start 2 to 3 days before departure. If diarrhea persists beyond 3 days, especially with fever or dehydration, escalate care.
Antifungal drugs like fluconazole, nystatin, or ketoconazole can inactivate S. boulardii, so do not take them together. People with central venous lines, those who are severely immunocompromised, or patients in intensive care should avoid live probiotics due to rare bloodstream infections. If you have a known yeast allergy, skip S. boulardii and choose a bacterial-only probiotic.
Skip self-treatment if you have high fever, bloody stools, signs of dehydration, severe abdominal pain, or diarrhea after recent hospitalization or chemotherapy. Pregnancy is generally considered compatible with probiotics, but persistent symptoms warrant medical evaluation. If your symptoms are chronic with weight loss or nighttime diarrhea, you need workup rather than a short probiotic course.
Frequently asked questions
How fast does Saccharomyces boulardii work for diarrhea?
Most people who respond notice improvement within 24 to 72 hours. If symptoms are not improving by day 3, or you develop fever, blood, or dehydration, seek care and consider stool testing.
Can I take this probiotic with antibiotics?
Yes. Take it at least 2 to 3 hours away from your antibiotic dose and continue for about a week after finishing antibiotics. This timing reduces antibiotic-associated diarrhea and helps restore balance.
Does S. boulardii help with C. diff?
It is used alongside standard therapy to lower recurrence risk by degrading C. difficile toxins and supporting local immunity. Do not use it as a stand‑alone treatment; C. diff needs prompt medical care.
Do I need to refrigerate this probiotic?
Check the label on your bottle. Many S. boulardii products are shelf-stable at room temperature, but heat above typical room conditions can reduce potency. Keep it dry and away from high heat.
Are there side effects with S. boulardii?
Most side effects are mild, like gas or bloating in the first few days. Serious infections are very rare but can occur in people with central lines or severe immunosuppression, who should avoid live probiotics.
Can I take this during travel to prevent diarrhea?
Yes. Start 2 to 3 days before travel and continue through the trip. It reduces the risk and severity of traveler’s diarrhea, especially when combined with safe food and water practices.
Does this probiotic colonize the gut permanently?
No. S. boulardii is transient. It helps while you take it, then clears within days. That is sufficient for most short-term goals like antibiotic-associated or traveler’s diarrhea.
Can I use this for IBS symptoms like bloating?
It can help some people after a gut infection, but evidence is stronger for acute diarrhea and antibiotic-associated diarrhea. For chronic IBS, consider a targeted bacterial probiotic or low FODMAP diet.
How to take it & ingredients
Suggested use: Take one capsule one to two times daily or as directed by your healthcare practitioner.
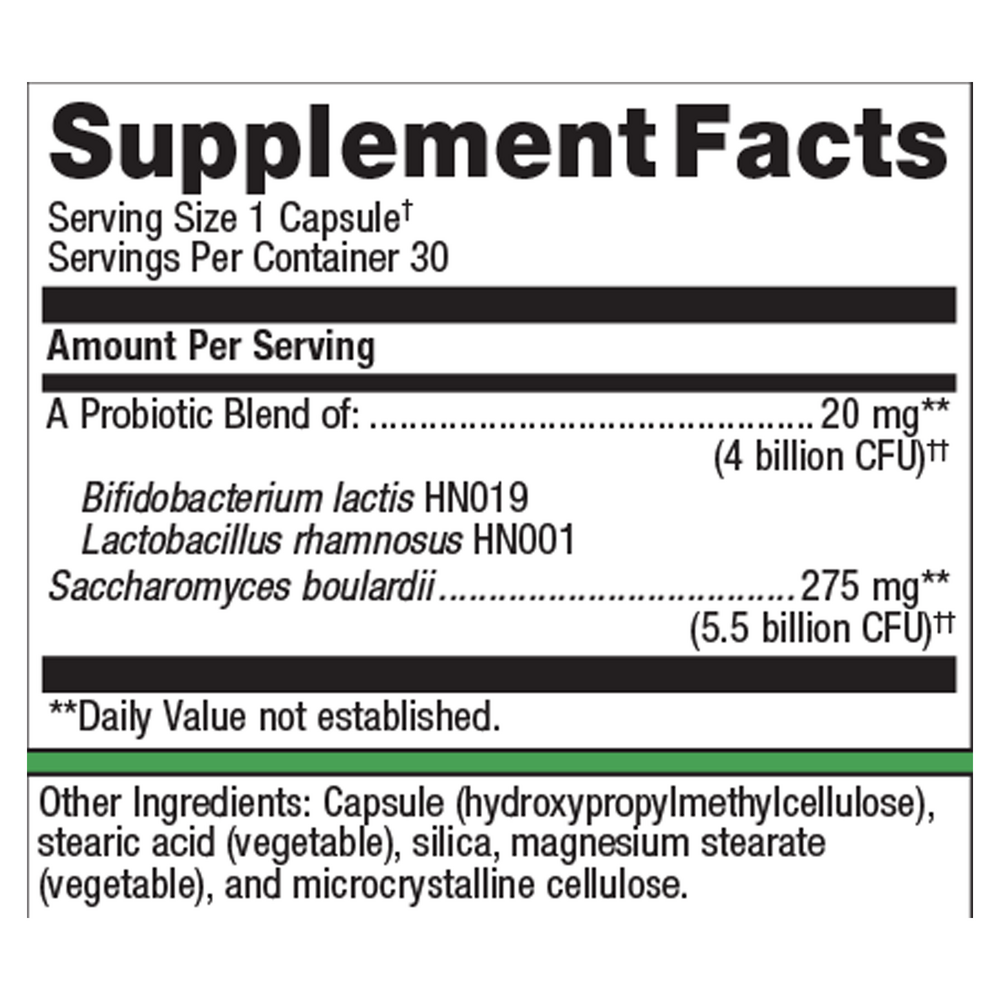
Active ingredients
1 capsule per serving · 30 servings
▼
Probiotic Blend
4 billion CFU, 20 mg
Bifidobacterium lactis HN019
-
Lactobacillus rhamnosus HN001
-
Saccharomyces boulardii
5.5 billion CFU, 275 mg
Other ingredients: Capsule (hydroxypropylmethylcellulose, sodium copper chlorophyllin), Stearic acid (vegetable), Silica, Magnesium stearate (vegetable), Microcrystalline cellulose
Certifications
Benefits
Warnings
Customers also considered

Thorne
Bacillus Coagulans
60 capsules
$XX.XX$33.00retail
Add to cart to see your price

Thorne
Complete Biotic
30 packets
$XX.XX$46.00retail
Add to cart to see your price
Dr. Mercola
Complete Probiotics 70 Billion CFU
30 capsules
$XX.XX$46.99retail
Add to cart to see your price
Garden of Life
Dr. Formulated Probiotics Mens Daily Care
30 capsules
$XX.XX$45.99retail
Add to cart to see your price