

Nature’s Way
Melatonin Lozenge 2.5 mg by Nature’s Way
100 lozenges · 100-day supply
Support Restful Sleep with Natural Melatonin Lozenge$9.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Dairy Free·Sugar Free·Wheat Free·Yeast Free·
Nature’s Way Melatonin Lozenge overview
If falling asleep is your bottleneck, melatonin 2.5 mg is a practical starting dose. It fits frequent travelers managing jet lag, night-shift workers trying to anchor a new schedule, and adults with delayed sleep timing who naturally fall asleep too late. It’s also reasonable if evening light exposure is hard to control. If you mainly wake up often at night, melatonin is less helpful than tightening sleep hygiene and checking contributors like caffeine or alcohol.
Melatonin is your brain’s dusk signal, not a sedative. Light hitting the eyes suppresses its release; darkness lets it rise, which cues the body to initiate sleep. Taking melatonin at night nudges this internal clock earlier, so you get sleepy closer to the target bedtime. A lozenge that dissolves in the mouth leads to faster absorption than a tablet you swallow, so onset can feel quicker. It can shorten time to sleep, but it won’t maintain sleep if other drivers keep you awake.
Let one lozenge dissolve 30–60 minutes before bed. For jet lag, take it at the destination’s bedtime, starting the first evening after arrival; eastbound trips often benefit from a night or two before travel. For night-shift anchoring, take it before the intended daytime sleep period in a darkened room. This is a mid-range dose; some adults do well with less, while persistent circadian issues sometimes need short-term higher dosing under clinician guidance.
Skip melatonin if you’re pregnant or breastfeeding. Use caution and speak with your clinician if you take warfarin or other blood thinners, fluvoxamine (it can raise melatonin levels), immunosuppressants after transplant, or sedatives. People with autoimmune disease, epilepsy, or severe depression should use medical guidance. If you feel groggy the next morning, take it earlier or lower the dose. Avoid alcohol near bedtime, and dim screens and overhead lights for best results.
Frequently asked questions
How fast does melatonin 2.5 mg work?
For sleep onset, most feel an effect within 30–60 minutes, especially with a lozenge that absorbs faster. Shifting your body clock for jet lag or delayed sleep timing takes several days of consistent timing and light control.
Can I take melatonin every night?
Yes, many adults use it nightly for timing the sleep window. If you need it long-term, pair it with strict light management and a fixed wake time. If you need higher and higher doses or still feel unrefreshed, evaluate for sleep apnea or restless legs.
What time should I take melatonin for jet lag?
Take it at your destination’s local bedtime. For eastbound trips, starting one to two evenings before departure can help. Combine with morning bright light at the destination and minimal light before bed for a stronger shift.
Does melatonin cause vivid dreams or grogginess?
It can. Vivid dreams are common when sleep deepens; morning grogginess often means the dose was too high or taken too late. Try an earlier time or a lower dose if you wake feeling foggy.
Is melatonin safe with antidepressants or anxiety meds?
Usually, but check first. Fluvoxamine can raise melatonin levels, and any sedative effect may add up with other calming medications. If you feel overly drowsy, reduce the dose or stop and speak with your prescriber.
Will melatonin help me stay asleep all night?
It mainly helps you fall asleep earlier and faster. If you wake frequently, look at alcohol, late fluids, reflux, pain, or sleep apnea. For middle-of-the-night waking, timing and environment changes usually outperform more melatonin.
Can I drive after taking melatonin?
No. Plan to be in for the night. Melatonin makes you sleepy and can slow reaction time. Take it when you are done driving and operating tools for the evening.
How to take it & ingredients
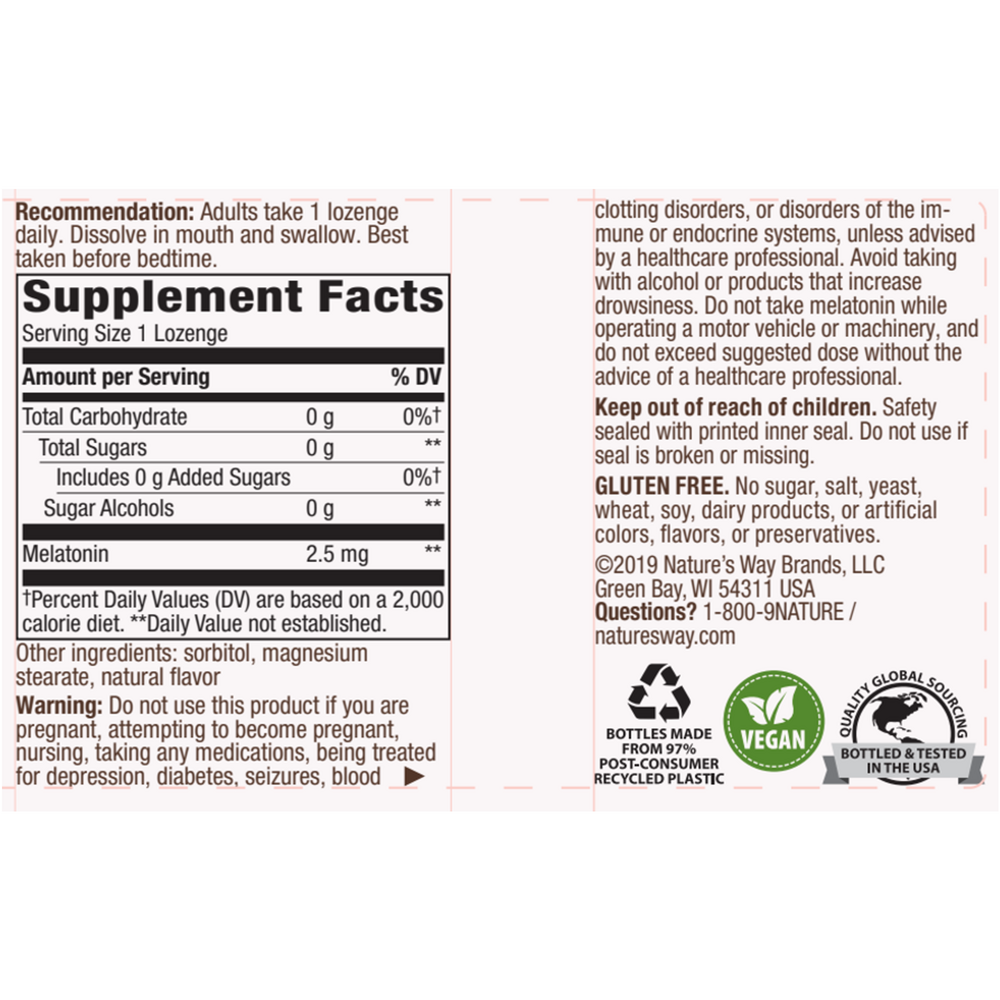
Suggested use: Adults take 1 lozenge daily. Dissolve in mouth and swallow. Best taken before bedtime.
Active ingredients
1 lozenge per serving · 100 servings
Melatonin
2.5 mg
Other ingredients: Sorbitol, Natural flavor, Magnesium stearate
Certifications
Benefits
Warnings



