


New Chapter
Wholemega 1000 mg by New Chapter
60 softgels · 30-day supply
Wild Alaskan Salmon Oil for Heart, Brain, and Joint Health$36.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Kosher·Gluten Free
New Chapter Wholemega 1000 mg overview
If you’re shopping for fish oil for triglycerides, this is better as a daily maintenance oil than a triglyceride-lowering therapy. Whole salmon oil with 520 mg omega-3s per softgel fits people with a low or low-normal Omega-3 Index, light seafood intake, or those wanting a whole-food-style oil. If your triglycerides are elevated, you’ll likely need a higher-dose omega-3 plan.
EPA and DHA reduce how much fat your liver packages into VLDL particles (the carriers that show up on a lipid panel as triglycerides) and nudge cells to burn fatty acids for energy. At higher intakes, responders often see triglycerides drop 20–30% within 4 to 12 weeks. This salmon oil also brings omega-7s, astaxanthin, and a trace of vitamin D3, which add antioxidant color but don’t replace a targeted dose for triglycerides or hs-CRP (an inflammation marker).
Take one softgel twice daily immediately before your two largest meals, as New Chapter suggests. Food, especially fat-containing meals, improves omega-3 absorption and reduces fishy burps. If your goal is a meaningful triglyceride drop, consider a concentrated fish oil delivering 2–4 grams of EPA+DHA per day or discuss prescription-grade options with your clinician.
Use caution if you’re on blood thinners like warfarin, apixaban, rivaroxaban, or clopidogrel; fish oil can modestly increase bleeding tendency. Pause before surgery if your surgeon advises. Skip if you have a fish allergy. For very high triglycerides, consider prescription icosapent ethyl (pure EPA) or a higher-dose EPA+DHA product alongside diet changes, then recheck triglycerides.
How fast will you feel it? Blood levels (Omega-3 Index) rise over 4–12 weeks; symptom changes are gradual. Is salmon oil better than concentrates? It’s a whole-food profile, but concentrates are more practical for triglyceride lowering. Is 1,000 mg fish oil enough? For maintenance, often yes; for triglycerides, usually not. Worried about burps? Take with meals and keep capsules cool.
Frequently asked questions
Does fish oil thin your blood?
Fish oil has a mild anti-platelet effect, which can increase bleeding tendency at higher intakes. It’s usually not clinically significant, but be cautious with warfarin, apixaban, rivaroxaban, or clopidogrel, and before surgery. Discuss dose with your clinician if you bruise easily or have bleeding risks.
How long does fish oil take to lower triglycerides?
With adequate dosing (typically 2–4 grams EPA+DHA daily), responders see triglycerides fall within 4–12 weeks. At about 1 gram per day, effects on triglycerides are modest. Recheck a lipid panel after 8–12 weeks to see your personal response and adjust the plan.
Is salmon oil as effective as concentrated fish oil?
For maintenance of the Omega-3 Index, salmon oil works well. For targeted triglyceride reduction, concentrated fish oil or prescription EPA is more efficient because it delivers higher EPA+DHA per capsule, which is what drives the lipid changes seen in trials.
Can I take fish oil with statins?
Yes. Fish oil and statins are often combined, and the effects on triglycerides can be additive. If you’re already on a statin, review your lipid goals with your clinician to choose an EPA/DHA dose that matches your targets and to avoid duplicating therapy.
What labs should I check with omega-3s?
Track your Omega-3 Index to confirm intake is landing in your tissues, and monitor triglycerides if that’s your goal. hs-CRP can reflect inflammation trends. Re-test after 8–12 weeks on a stable dose, then every few months once you’re steady.
Will this help with joint or skin health?
Some people notice milder morning stiffness or drier-skin relief over several weeks, likely from membrane effects of EPA/DHA. These outcomes are variable and dose-dependent. If joints are your main goal, consider staying consistent for 2–3 months before judging.
What if fish oil upsets my stomach?
Take capsules just before meals, not on an empty stomach. Splitting doses, keeping them cold, and starting with one capsule daily for a week can help. If burps persist, try enteric-coated or triglyceride-form concentrates, or switch brands.
How to take it & ingredients
Suggested use: Take one softgel two times daily, preferably immediately before your two largest meals, or as recommended by your healthcare professional.
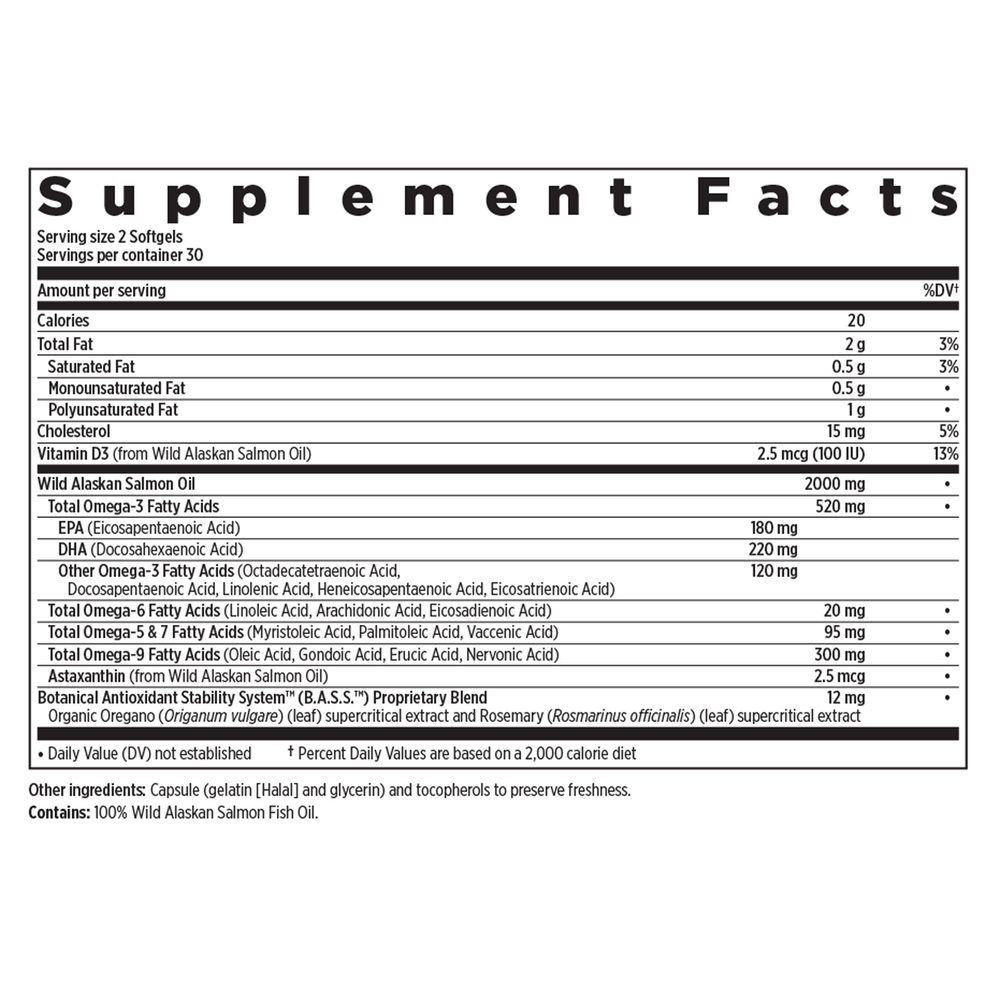
Active ingredients
2 softgels per serving · 30 servings
▼
Total Omega-3 Fatty Acids
520 mg
Eicosapentaenoic Acid (EPA)
180 mg
Docosahexaenoic Acid (DHA)
220 mg
Other Omega-3 Fatty Acids
Octadecatetraenoic Acid, Docosapentaenoic Acid, Linolenic Acid, Heneicosapentaenoic Acid, Eicosatrienoic Acid
Octadecatetraenoic Acid, Docosapentaenoic Acid, Linolenic Acid, Heneicosapentaenoic Acid, Eicosatrienoic Acid
120 mg
Total Omega-6 Fatty Acids
Linoleic Acid, Arachidonic Acid, Eicosadienoic Acid
Linoleic Acid, Arachidonic Acid, Eicosadienoic Acid
20 mg
Total Omega-5 & 7 Fatty Acids
Myristoleic Acid, Palmitoleic Acid, Margaroleic Acid
Myristoleic Acid, Palmitoleic Acid, Margaroleic Acid
95 mg
Total Omega-9 Fatty Acids
Oleic Acid, Gadoleic Acid, Erucic Acid, Nervonic Acid
Oleic Acid, Gadoleic Acid, Erucic Acid, Nervonic Acid
300 mg
Vitamin D3
From Wild Alaskan Salmon Oil
From Wild Alaskan Salmon Oil
2.5 mcg, 100 IU
Astaxanthin
From Wild Alaskan Salmon Oil
From Wild Alaskan Salmon Oil
2.5 mcg
Botanical Antioxidant Stability System (B.A.S.S.™) Proprietary Blend
Organic Oregano (leaf) and Rosemary (leaf) supercritical extracts
Organic Oregano (leaf) and Rosemary (leaf) supercritical extracts
12 mg
Other ingredients: Capsule (Gelatin [Halal] and Glycerin), Tocopherols (to preserve freshness)
Certifications
Benefits
Warnings
Customers also considered

Thorne
Advanced DHA
60 gelcaps
$30.00extra 10% off with Subscribe & Save

Garden of Life
Dr. Formulated Advanced Omega
60 softgels
$31.99extra 19% off with Subscribe & Save
Garden of Life
Dr. Formulated DHA 1g
30 softgels
$31.99extra 19% off with Subscribe & Save
Garden of Life
Dr. Formulated Prenatal DHA
30 softgels
$29.99extra 20% off with Subscribe & Save