
Nordic Naturals
Ultimate Omega Plant Based 1210 mg by Nordic Naturals
60 softgels · 30-day supply
Plant-Based Omega-3s for Heart, Brain, and Overall Wellness$48.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Gluten Free·Soy Free·Milk Free·Wheat Free·Artificial Color Free
Nordic Naturals Ultimate Omega Plant Based overview
If you avoid fish but want EPA and DHA omega-3, this algae-based option fits. It’s useful if your Omega-3 Index (a blood test of EPA+DHA in red cells) is low or in the lower normal range, if you’re planning pregnancy and not eating seafood, or if you’re a vegan on a restrictive diet. At 1,210 mg total omega-3s per day, it’s a solid maintenance dose; if your triglycerides are elevated, higher EPA+DHA intakes are typically needed for reduction under clinician guidance.
EPA and DHA reduce how much fat your liver exports in VLDL particles (the form that shows up as triglycerides on a lipid panel), and they nudge cells to burn fatty acids for energy faster. Most responders see triglycerides fall within 4 to 12 weeks. These fats also shift the signaling molecules your cell membranes make, which explains the modest drops in hs-CRP (a marker of inflammation) seen in some people. Algae oil delivers preformed EPA and DHA directly, unlike ALA from flax or chia, which converts poorly.
Take two softgels daily with food, ideally with a meal that contains fat for better absorption. If you’re sensitive to burps, split the dose with breakfast and dinner. Recheck your Omega-3 Index after 8 to 12 weeks to confirm you’re where you want to be. If you’re targeting triglyceride lowering rather than maintenance, discuss a higher total EPA+DHA plan with your clinician.
Omega-3s can modestly increase bleeding time. If you take blood thinners like warfarin, apixaban, rivaroxaban, or antiplatelet drugs like clopidogrel, coordinate dosing with your prescriber and monitor for bruising or nosebleeds. If you have a history of fish or shellfish allergy, algae oil is generally well tolerated, but check the label for cross-contact. For upcoming surgery, most surgeons ask patients to pause omega-3s 3 to 7 days beforehand.
Frequently asked questions
Is vegan omega-3 as effective as fish oil?
Yes, if it delivers similar amounts of EPA and DHA. Algae oil provides the same molecules found in fish oil, so blood levels (Omega-3 Index) and triglyceride responses track with dose, not the source.
How long does omega-3 take to work?
Expect changes in triglycerides and the Omega-3 Index within 4 to 12 weeks. Cell membranes turn over gradually, so consistency matters; take it daily with meals and reassess after about 2 to 3 months.
Can I rely on flax or chia instead of algae omega-3?
Usually not for targeted goals. ALA from plants converts poorly to EPA and DHA in adults. If your Omega-3 Index is low or you’re aiming to lower triglycerides, direct EPA+DHA sources work better.
Does omega-3 thin your blood?
It doesn’t “thin” blood like a prescription anticoagulant, but it can slightly increase bleeding time. The effect is small for most people, but coordinate with your prescriber if you’re on blood thinners.
What side effects should I watch for with omega-3?
The most common are fishy burps, mild stomach upset, or loose stools. Taking it with food, splitting doses, or storing softgels in the freezer usually fixes this. Persistent GI issues warrant a dose adjustment.
What labs should I check with omega-3?
Track the Omega-3 Index to ensure repletion, and triglycerides if that’s your goal. In inflammation-driven conditions, hs-CRP can be followed, though reductions are modest and not universal.
Is this dose enough to lower high triglycerides?
It’s a maintenance-level dose. Triglyceride lowering typically needs higher total EPA+DHA than provided here. Work with your clinician on dosing and retest lipids after 8 to 12 weeks.
How to take it & ingredients
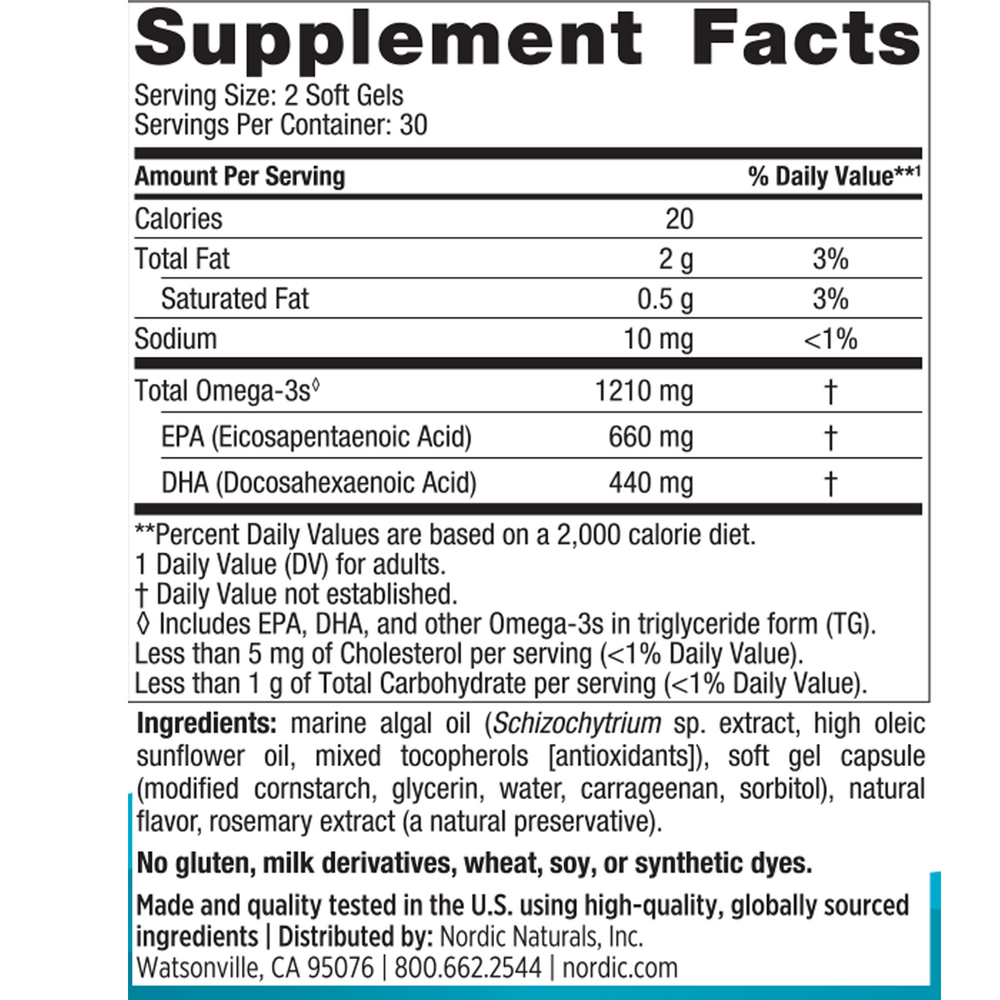
Suggested use: Adults take two softgels daily with food, or as directed by your healthcare professional.
Active ingredients
2 softgels per serving · 30 servings
▼
Total Omega-3s
1210 mg
EPA
Eicosapentaenoic acid
Eicosapentaenoic acid
660 mg
DHA
Docosahexaenoic acid
Docosahexaenoic acid
440 mg
Other ingredients: High oleic sunflower oil, Mixed tocopherols (antioxidants), Softgel capsule (modified cornstarch, glycerin, water, carrageenan, sorbitol), Natural flavor, Rosemary extract (natural preservative)
Certifications
Benefits
Warnings
Customers also considered

Nordic Naturals
Algae Omega
60 softgels
$30.99extra 19% off with Subscribe & Save

Body Bio
BodyBio Balance Oil
473 milliliters
$36.99extra 19% off with Subscribe & Save

Pure Encapsulations
EPO
100 softgels
$33.00extra 21% off with Subscribe & Save

Barlean's Organic Oils
Evening Primrose Oil
120 softgels
$39.99extra 20% off with Subscribe & Save