


Nordic Naturals
Vitamin D3 Gummies 1000 IU by Nordic Naturals
120 gummies · 120-day supply
Delicious Gummies for Bone Health and Immune Support$21.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Artificial Color Free·Artificial Flavor Free
Nordic Naturals Vitamin D3 Gummies overview
If your Vitamin D, 25-Hydroxy is in the lower part of the normal range and you want simple maintenance, vitamin D3 gummies at 1,000 IU fit well. They’re a practical choice if you get little sun, have darker skin, consistently use sunscreen, work indoors at northern latitudes, or maintain low‑fat or dairy‑free diets. People with higher body weight often need more than 1,000 IU for the same effect. For clearly low levels, this maintenance dose is usually too small for repletion—use higher dosing under clinician guidance, then step down.
D3 (cholecalciferol) is the form your skin makes from sunlight, and it’s better at raising blood levels than D2 (ergocalciferol). Your liver and kidneys convert it into the active hormone that increases calcium absorption from the gut and helps regulate bone turnover. Adequate D3 keeps parathyroid hormone (the signal that pulls calcium from bone) in check. Interest in vitamin D for preventing infections was high during COVID, but large randomized trials show only modest or no benefit for most people who aren’t deficient.
Take one gummy daily with food, ideally a meal that contains some fat to improve absorption. Time of day is flexible—pick a time you’ll remember. If your level was low and you’ve adjusted dosing, recheck Vitamin D, 25-Hydroxy within 8 to 12 weeks to confirm you’ve landed in your target range, then continue maintenance. If you routinely miss days, weekly catch‑up is reasonable, but avoid stacking large amounts without level monitoring.
Skip or get medical guidance if you have a history of high calcium, recurrent kidney stones, sarcoidosis or other granulomatous disease (conditions that can overproduce active vitamin D), or severe kidney disease. Thiazide diuretics (blood‑pressure meds that reduce calcium loss) raise the risk of high calcium when paired with high‑dose D. Orlistat and cholestyramine (fat‑blocking and bile‑acid–binding drugs) reduce absorption—separate timing by several hours. Long‑term steroids increase vitamin D needs, so lab‑guided dosing matters.
Frequently asked questions
Is 1,000 IU vitamin D3 enough?
It’s a maintenance dose for many adults whose Vitamin D, 25-Hydroxy is low‑normal. If your level is clearly low, repletion typically requires higher daily or weekly doses under clinician guidance, followed by 1,000–2,000 IU for upkeep.
How long do vitamin D3 gummies take to work?
Blood levels usually rise within 4 to 12 weeks. If you started low or have higher body weight, the climb is slower and you may need a larger dose initially. Recheck Vitamin D, 25-Hydroxy after 8–12 weeks to verify your response.
Do I need to take vitamin D3 with fat?
Yes, taking D3 with a meal that includes fat improves absorption. If you eat very low‑fat, consider pairing your gummy with foods like eggs, yogurt, olive oil, or nuts to make the dose more reliable.
Should I pair vitamin D3 with vitamin K2?
K2 is helpful for bone if your overall intake is low, but it’s not required to absorb or use vitamin D3. If you’re on warfarin (a blood thinner that targets vitamin K), avoid extra K2 unless your prescriber approves.
Can I take vitamin D3 gummies at night?
Any time works. Some people prefer morning with breakfast for consistency. If you notice sleep changes, shift to earlier in the day, but most do not experience sleep effects with D3.
Are vitamin D3 gummies safe in pregnancy?
Yes in typical maintenance doses, but pregnancy needs vary. Ask your obstetric clinician and check Vitamin D, 25-Hydroxy to individualize dosing rather than guessing, especially if your level was low before pregnancy.
What are common side effects of vitamin D3?
At maintenance doses, side effects are uncommon. Very high intakes over time can raise calcium, causing thirst, frequent urination, or nausea. That’s why dose adjustments should follow lab results, not guesswork.
How to take it & ingredients
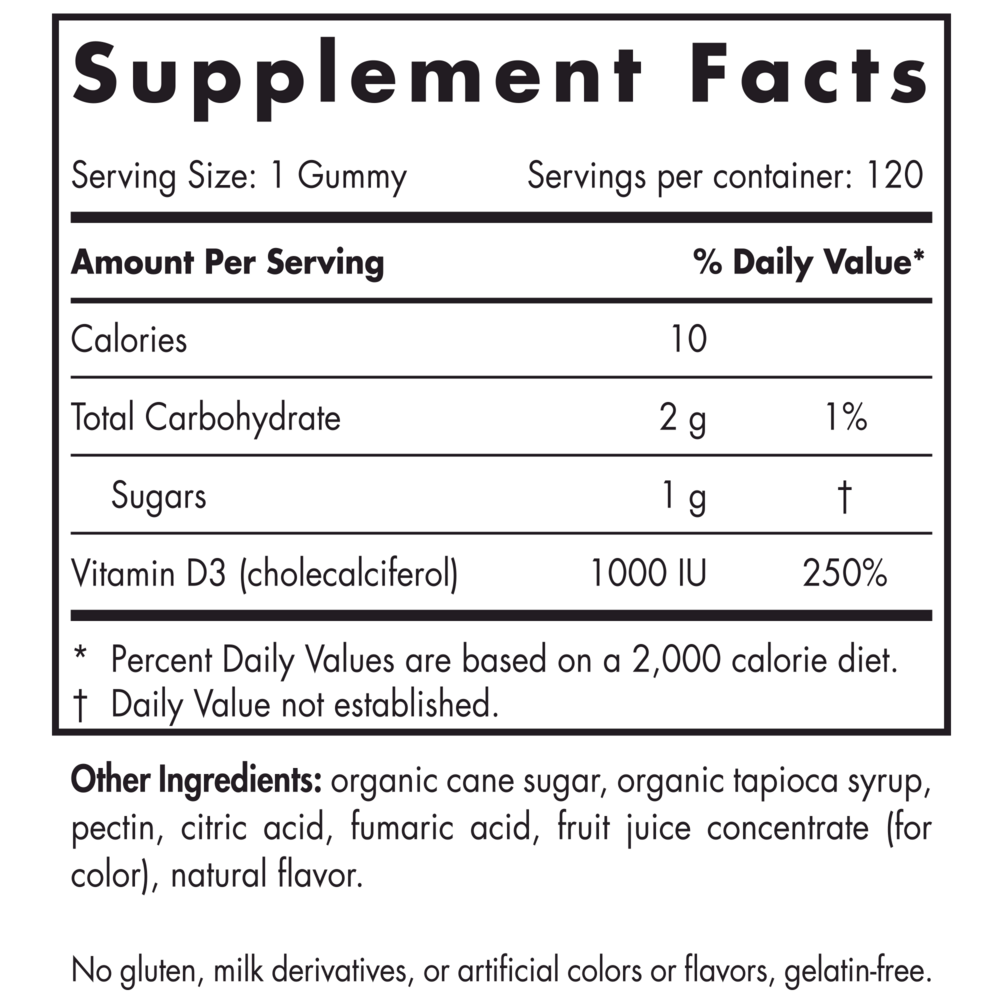
Suggested use: One gummy daily, with food, or as directed by your health care professional or pharmacist.
Active ingredients
1 gummy per serving · 120 servings
Vitamin D
D3 (Cholecalciferol)
D3 (Cholecalciferol)
1000 IU
Other ingredients: Organic Cane Sugar, Organic Tapioca Syrup, Pectin, Citric Acid, Fumaric Acid, Fruit Juice Concentrate (for color), Natural Flavor
Certifications
Benefits
Warnings



