


Nordic Naturals
Vitamin D3 Gummies 1000 IU by Nordic Naturals
60 gummies · 60-day supply
Delicious Gummies for Healthy Bones and Immune Support$14.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Artificial Color Free·Artificial Flavor Free
Nordic Naturals Vitamin D3 Gummies overview
If your Vitamin D, 25-Hydroxy is in the lower end of the normal range and you want a simple maintenance dose, vitamin D3 gummies at 1,000 IU fit well. They suit darker‑skinned adults, people who get little midday sun, sunscreen users, and those at northern latitudes. Higher body weight often calls for more than 1,000 IU. If your level is meaningfully low, this dose is usually too light for repletion; correct under clinician guidance, then use vitamin D3 gummies for upkeep.
Vitamin D3 (cholecalciferol) is the form your skin makes from sunlight, and it raises Vitamin D, 25-Hydroxy more reliably than D2 (ergocalciferol). Your liver and kidneys convert D3 into its active hormone, which increases calcium absorption from the gut and tempers parathyroid hormone (the signal that pulls calcium from bone). That combination stabilizes bone turnover. Hopes that vitamin D prevents infections haven’t held up in large trials, so take vitamin D3 gummies for bone and metabolic needs, not for cold season insurance.
Take one vitamin D3 gummy with food, ideally a meal containing some fat, since vitamin D is fat‑soluble and absorbs better that way. Recheck Vitamin D, 25-Hydroxy after 8–12 weeks to confirm you’re in range and adjust. If you routinely need more than 1,000 IU for maintenance, a higher‑strength vitamin D3 softgel is more practical. Pairing with calcium isn’t required; dose calcium only if your diet is low and your calcium goals aren’t met with food.
Avoid unsupervised vitamin D3 if you have a history of high calcium, recurrent kidney stones, sarcoidosis or other granulomatous disease (conditions that can drive excess active vitamin D), or primary hyperparathyroidism. Review meds that change vitamin D handling: orlistat (fat‑blocking) reduces absorption, chronic steroids and some seizure medicines lower levels, and thiazide diuretics can raise calcium. In these cases, coordinate dosing and monitor Calcium and Vitamin D, 25-Hydroxy.
Frequently asked questions
How long do vitamin D3 gummies take to raise my levels?
Most people see Vitamin D, 25-Hydroxy move meaningfully within 8–12 weeks. Recheck then and adjust. If your starting level is very low or body weight is higher, expect to need a larger dose initially under clinician guidance.
Should I take vitamin D3 with food or on an empty stomach?
Take vitamin D3 with food, ideally one that contains some fat, to improve absorption. Morning or evening both work—consistency matters more than timing.
Can vitamin D3 gummies replace sunlight?
They can maintain Vitamin D, 25-Hydroxy when sun exposure is limited. Sunlight has other effects (like setting circadian rhythm), so aim for light exposure for sleep and mood, and use vitamin D3 to cover your blood level.
Do vitamin D3 gummies cause side effects?
At maintenance doses like 1,000 IU, side effects are uncommon. Very high intakes over time can raise calcium, causing thirst, nausea, or fatigue. If you have a history of high calcium or kidney stones, get labs and medical guidance.
Is 1,000 IU of vitamin D3 enough?
It’s a maintenance dose for many with low‑normal Vitamin D, 25-Hydroxy. If your level is low, you’ll likely need a higher repletion plan, then step down to 1,000 IU. Higher body weight or minimal sun often requires more for upkeep.
What medications interact with vitamin D3?
Orlistat can reduce absorption; chronic steroids and some seizure drugs lower vitamin D levels; thiazide diuretics can raise calcium. If you use these, coordinate dosing and monitor Vitamin D, 25-Hydroxy and Calcium with your clinician.
Can I take vitamin D3 with magnesium or calcium?
Yes. Magnesium helps enzymes activate vitamin D, and many diets fall short. Calcium isn’t required with vitamin D; add it only if your dietary intake is low or your labs and bone goals call for it.
How to take it & ingredients
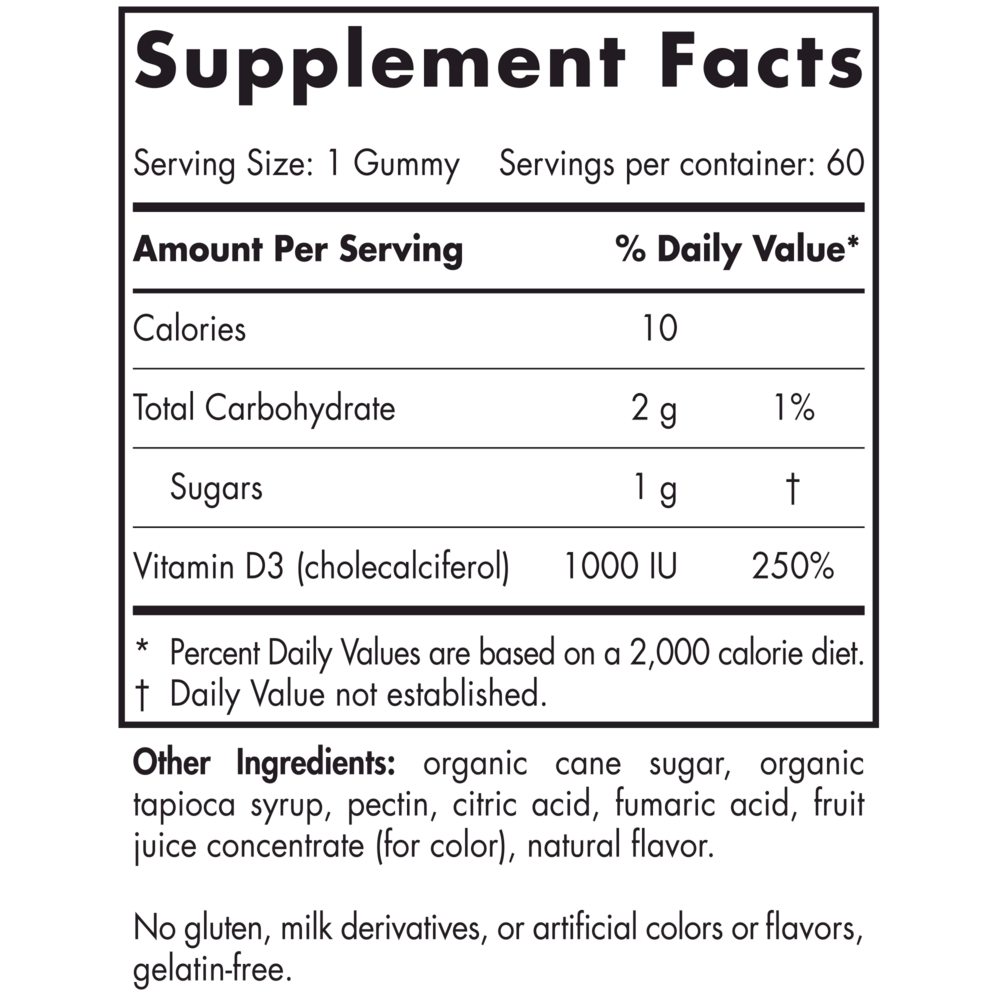
Suggested use: One gummy daily, with food, or as directed by your health care professional or pharmacist.
Active ingredients
1 gummy per serving · 60 servings
Vitamin D
D3 (Cholecalciferol)
D3 (Cholecalciferol)
1000 IU
Other ingredients: Organic Cane Sugar, Organic Tapioca Syrup, Pectin, Citric Acid, Fumaric Acid, Fruit Juice Concentrate (for color), Natural Flavor
Certifications
Benefits
Warnings



