

Ortho Molecular Products
Reacted Calcium by Ortho Molecular Products
180 capsules · 90-day supply
Comprehensive Calcium Support for Bone Health and Strength$63.88
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Reacted Calcium overview
If you are looking for a calcium supplement for bone density because your DXA scan showed decline or your dietary calcium is low, this fits. It is practical for post‑menopausal women, adults on acid‑blocking meds, people who avoid dairy, and long‑term steroid users. Check Vitamin D, 25-Hydroxy first; if your level is low, fixing vitamin D improves how well calcium builds bone. Count food intake, then use supplements to close the gap rather than overshoot.
This formula blends four forms: calcium citrate, dicalcium malate, calcium bisglycinate (a chelated form bound to the amino acid glycine for easier uptake), and microcrystalline hydroxyapatite (the calcium‑phosphorus mineral your bones are made of). Multiple forms improve absorption even with reduced stomach acid. Calcium, with vitamin D3, lowers parathyroid hormone (the signal that pulls calcium from bone), helping you maintain bone over time. Expect changes on bone markers and scans over months, not weeks.
Per label, take 1–2 capsules three times daily, ideally with meals. The critical rule is dose size: the gut absorbs calcium best in divided amounts around 500–600 mg elemental at a time. This product provides 500 mg per serving, so spread intake across the day. Separate calcium by 2–4 hours from iron, levothyroxine, tetracyclines or fluoroquinolone antibiotics, and bisphosphonates. If you use a proton‑pump inhibitor, citrate and bisglycinate remain well absorbed with meals.
Skip supplementation and speak with your clinician if you have a history of high blood calcium, recurrent kidney stones, sarcoidosis, primary hyperparathyroidism, or advanced kidney disease. Thiazide diuretics can raise calcium levels; monitor if you use them. For stone‑formers who still need calcium, take it with meals and discuss a 24‑hour urine calcium test. Constipation is the most common side effect; increase fluids, fiber, and magnesium if needed.
Frequently asked questions
How much calcium should I take per day?
Count food first, then supplement only the gap. Most adults need roughly 1,000–1,200 mg total intake daily from diet plus supplements. Avoid taking more than about 500–600 mg elemental at one time because absorption drops with larger single doses.
Is calcium citrate better than other forms?
Citrate is absorbed well even with low stomach acid and tends to be gentler on the gut. This blend also includes bisglycinate, dicalcium malate, and hydroxyapatite to cover different uptake routes. Carbonate requires more stomach acid and can cause more gas for some people.
Do I need vitamin D with calcium?
Yes, vitamin D makes calcium usable. This formula includes 10 mcg (400 IU) of vitamin D3, which is a maintenance amount. If your Vitamin D, 25-Hydroxy is low, you will likely need a higher D3 dose temporarily under clinician guidance, then step down.
How long until calcium affects bone density?
Bone changes slowly. Expect months to a year to see effects on a DXA scan. Consistent calcium, adequate vitamin D, protein intake, and resistance training are the levers that move bone the most. Short trials rarely show meaningful changes.
Does calcium cause kidney stones?
Dietary calcium with meals generally lowers oxalate absorption and can reduce certain stone risks. High-dose calcium supplements between meals can raise risk in susceptible people. If you have a stone history, take calcium with food and ask about a 24‑hour urine evaluation.
Does calcium increase heart attack risk?
Data are mixed. Large food‑first calcium intake looks neutral, while some studies raised concern with high-dose supplements. A practical approach is to meet most needs from diet, then use divided, meal‑time doses to fill gaps rather than large boluses.
Can I take calcium with PPIs or H2 blockers?
Yes. Calcium citrate and bisglycinate are absorbed even with low stomach acid. Take with meals and split doses across the day. Avoid carbonate if you have persistent low acid, as it depends more on stomach acid for absorption.
What interacts with calcium supplements?
Calcium binds many drugs and minerals. Separate by 2–4 hours from iron, levothyroxine, tetracycline or fluoroquinolone antibiotics, and bisphosphonates. Thiazide diuretics can raise blood calcium; monitor with your clinician if you use them.
How to take it & ingredients
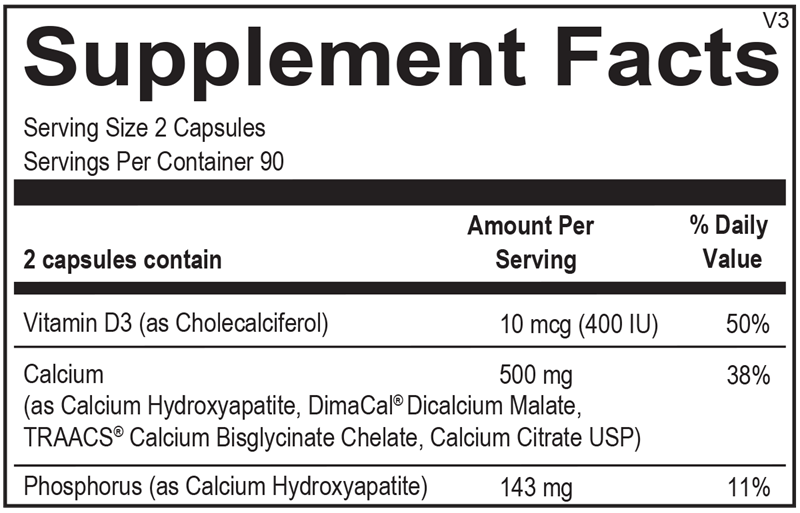
Suggested use: Take 1-2 capsules three times per day or as recommended by your health care professional.
Active ingredients
2 capsules per serving · 90 servings
Calcium
Calcium Hydroxyapatite, DimaCal® Dicalcium Malate, TRAACS® Calcium Bisglycinate Chelate, Calcium Citrate USP
Calcium Hydroxyapatite, DimaCal® Dicalcium Malate, TRAACS® Calcium Bisglycinate Chelate, Calcium Citrate USP
500 mg
Vitamin D3
Cholecalciferol
Cholecalciferol
10 mcg, 400 IU
Phosphorus
As Calcium Hydroxyapatite
As Calcium Hydroxyapatite
143 mg
Other ingredients: Natural Vegetable Capsules, Microcrystalline Cellulose, Magnesium Stearate, Silicon Dioxide
Certifications
Benefits
Warnings
Customers also considered

Thorne
Calcium
120 capsules
$28.00extra 10% off with Subscribe & Save

Klean Athlete
Calcium Citrate
120 capsules
$22.50extra 20% off with Subscribe & Save

Pure Encapsulations
Calcium Citrate
180 capsules
$32.50extra 20% off with Subscribe & Save
Solaray
Calcium Citrate 1g
240 capsules
$26.99extra 19% off with Subscribe & Save