


Pure Encapsulations
Vitamin D3 Liquid 1000 IU (25 mcg) by Pure Encapsulations
22.5 milliliters
Essential Vitamin D3 for Bone, Immune, and Mood Support$33.00
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegetarian·Gluten Free
Pure Encapsulations Vitamin D3 Liquid overview
If you’re searching for vitamin D3 drops to maintain a healthy Vitamin D, 25-Hydroxy level, this format fits. It suits adults with low sun exposure, darker-skinned adults at northern latitudes, people who consistently use sunscreen, and kids who need a small, flexible dose. It’s also practical if you dislike pills or want precise titration. This is a maintenance-level dose; if your level is meaningfully low or you have higher body weight, you’ll likely need a higher repletion plan first, then step down.
Cholecalciferol (vitamin D3) is the form your skin makes from sunlight and is more effective than D2 for raising blood levels. Your liver and kidneys convert it to the active hormone that boosts calcium absorption from the gut and helps keep parathyroid hormone (the signal that pulls calcium from bone) in check. That’s why bone density and fracture risk track with adequate D status. The buzz about D preventing infections was overstated; large randomized trials showed modest or no effect on most respiratory infections.
Take drops with food that contains fat for better absorption. Each drop provides 1,000 IU; the suggested use is 1–2 drops daily for ages 3–8 and 1–4 drops for ages 9 and up, or as directed by your clinician. Place drops on a spoon, then swallow—don’t aim the bottle directly into a child’s mouth. Recheck Vitamin D, 25-Hydroxy after 8–12 weeks to confirm you’re on target, and adjust the daily drop count based on your result and body weight.
Avoid unsupervised vitamin D3 if you have a history of high calcium, recurrent kidney stones, primary hyperparathyroidism, sarcoidosis or other granulomatous diseases, or severe kidney disease. Thiazide diuretics (blood pressure drugs that reduce calcium loss) raise the risk of high calcium on D. Orlistat and bile acid sequestrants can reduce absorption, and long-term steroids can blunt effects, so you may need monitoring of Calcium, PTH, and Vitamin D, 25-Hydroxy.
Frequently asked questions
How long do vitamin D3 drops take to raise levels?
Most people see Vitamin D, 25-Hydroxy rise within 4–12 weeks. The timeline depends on your starting level, body weight, dose per day, and whether you take it with food that contains fat.
Do I need vitamin K2 with vitamin D3?
You don’t need K2 to absorb vitamin D3. K2 is sometimes paired with higher-dose D or calcium regimens to influence calcium handling, but evidence for added benefit in routine maintenance dosing is mixed.
What’s the best time to take vitamin D3 drops?
Take vitamin D3 with your largest meal or any meal containing fat to improve absorption. Morning or evening is fine; consistency and taking it with food matter more than clock time.
Are vitamin D3 drops safe for kids?
Yes at appropriate doses. The suggested range here is 1–2 drops daily for ages 3–8 and 1–4 drops for ages 9+. For young children, confirm dosing with a pediatric clinician and avoid high-dose repletion without guidance.
Can I take vitamin D3 on an empty stomach?
You can, but absorption is better with food that contains fat. If you take it fasting, you may need a higher daily dose to achieve the same Vitamin D, 25-Hydroxy result.
What are signs of too much vitamin D3?
Symptoms come from high calcium: thirst, frequent urination, constipation, nausea, or confusion. If you notice these, stop and check Calcium and Vitamin D, 25-Hydroxy with your clinician.
Is liquid vitamin D3 vegan?
Vitamin D3 is often derived from lanolin (sheep’s wool), while some brands use lichen for a vegan source. Check the label or contact the manufacturer if you require a vegan-certified D3.
Can I rely on sun instead of vitamin D3 drops?
Sunlight can raise D, but season, latitude, skin tone, clothing, and sunscreen make it unreliable. If your Vitamin D, 25-Hydroxy runs low, a steady oral dose is a controllable way to maintain levels.
How to take it & ingredients
Suggested use: As a dietary supplement, children ages 3-8, take 1-2 drops daily. Adults and children ages 9 and up, take 1-4 drops daily, or as directed by a health professional. Consume with food.
Active ingredients
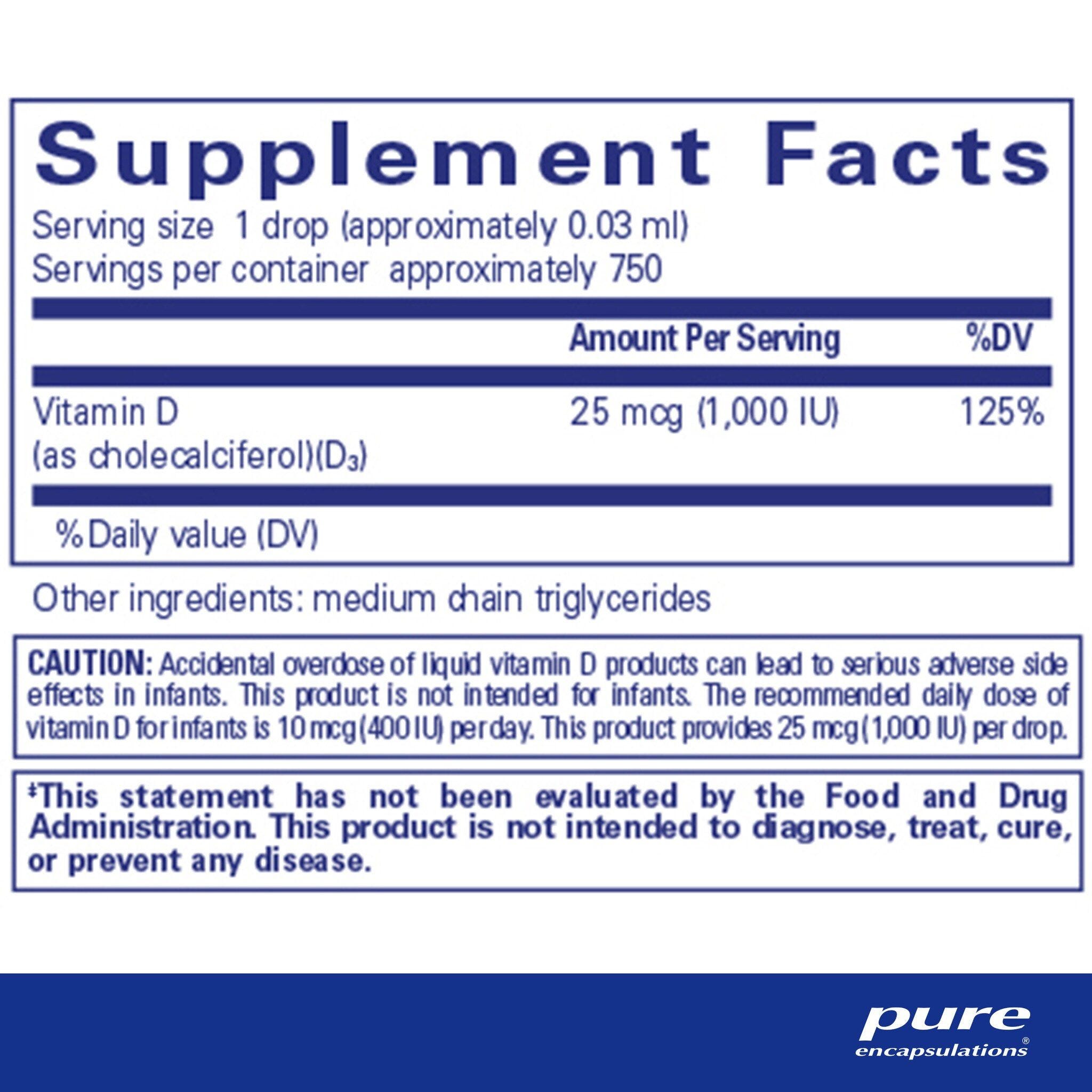
1 drop (~0.03 ml) per serving
Vitamin D
Cholecalciferol (D3)
Cholecalciferol (D3)
1000 IU, 25 mcg
Other ingredients: Medium Chain Triglycerides
Certifications
Benefits
Warnings



