


Pure Encapsulations
Digestive Enzymes Ultra 391 mg by Pure Encapsulations
180 capsules · 90-day supply
Comprehensive Support for Healthy Digestion and Nutrient Absorption$66.50
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegetarian·Gluten Free·Egg Free·Artificial Preservative Free·Peanut Free·Wheat Free·
Pure Encapsulations Digestive Enzymes Ultra overview
If you get post‑meal bloating, gas, or a heavy feeling after high‑fat, high‑protein, dairy, or bean-heavy meals, digestive enzymes are a practical first test. They’re helpful if you notice issues after starting a proton‑pump inhibitor (acid blocker), in midlife when stomach acid and pancreatic output trend lower, or after gallbladder removal. If your Omega-3 Index or hs-CRP aren’t the issue and symptoms are meal‑linked, this is a better knob to turn. For persistent fatty stools or weight loss, get checked for pancreatic insufficiency with a Fecal elastase test before self‑treating.
This blend supplies the enzymes your own pancreas and small intestine use to finish digestion. Proteases break proteins into absorbable amino acids, lipase splits fats so they don’t linger as greasy stools, and amylase turns starch into simpler sugars. Lactase targets milk sugar, often easing dairy-related gas. Alpha‑galactosidase helps with beans and cruciferous vegetables by reducing the carbs that gut bacteria ferment into gas. By reducing undigested leftovers, these enzymes can improve comfort and modestly improve nutrient absorption, which you’ll often notice as less bloating within the first few meals.
Take 1 capsule with the first bite of a meal; use 2 with larger, higher‑fat or dairy-heavy meals. For small snacks, many skip or use 1. Effects are meal‑to‑meal, so you can target problem meals. Give it 1 to 2 weeks of regular use to judge. If you routinely need more than 2 per meal or still see oily stools, ask your clinician about Fecal elastase, stool fat, or a lactose hydrogen breath test. Pure Encapsulations uses vegetarian enzymes, so they’re suitable if you avoid animal products.
Alpha‑galactosidase and other carb‑splitting enzymes can reduce the effect of acarbose or miglitol (diabetes drugs that slow carb absorption). Lipase can counteract orlistat (the fat‑blocking drug). If you use these, don’t combine without clinician guidance. People with a history of pancreatitis, active peptic ulcers, or severe food allergies should be cautious. If celiac disease is a question, get celiac serology (tTG IgA) rather than masking symptoms. Enzymes are generally well tolerated; mild nausea or loose stools usually resolve by lowering the dose or taking strictly with food.
Skip self‑treatment and get evaluated if you have red flags: unintended weight loss, anemia, chronic diarrhea, nighttime symptoms, or persistent fatty, floating stools. Those point to conditions that need testing and targeted therapy. After gallbladder removal, enzymes may help, but bile salts are sometimes the missing piece for fat tolerance—ask your clinician. During pregnancy, safety data for high‑potency proteases are limited; stick to diet changes and discuss any enzyme use with your obstetric clinician.
Frequently asked questions
Do digestive enzymes help with bloating and gas?
Often yes, when symptoms are tied to meals. Enzymes reduce undigested carbs, fats, and proteins that bacteria ferment into gas. If bloating is constant or occurs overnight, look beyond enzymes and discuss breath testing or stool studies.
How fast do digestive enzymes work?
You can notice less gas or heaviness at the very first meal. Give it 1–2 weeks of regular use to judge patterns and meal sizes. If there’s no change and fatty stools persist, ask about Fecal elastase or stool fat testing.
Can I take digestive enzymes with probiotics?
Yes. They act in different places: enzymes break down food in the gut lumen, while probiotics modulate the microbiome. Many people use both, taking enzymes at meals and probiotics away from food or at bedtime.
Can I use digestive enzymes if I’m on a PPI like omeprazole?
Yes. Acid blockers reduce stomach acidity, which can slow protein and mineral digestion; adding enzymes at meals can help with post‑meal fullness. If reflux worsens, reassess timing and meal size with your clinician.
Are digestive enzymes safe to take long term?
Generally yes when taken with food and at meal‑sized doses. If you become dependent for basic tolerance of everyday meals, investigate root causes such as lactose intolerance, celiac serology (tTG IgA), or pancreatic function.
Do digestive enzymes interfere with diabetes meds like acarbose?
They can. Carb‑digesting enzymes (like alpha‑galactosidase) may blunt the drug’s effect of slowing carbohydrate absorption. If you use acarbose or miglitol, consult your prescriber before adding enzymes.
What are common side effects of digestive enzymes?
Mild nausea, loose stools, or cramping can occur, usually from taking them on an empty stomach or overdosing for the meal size. Take with the first bite and reduce the dose. Stop and seek care if symptoms are severe.
Will digestive enzymes help after gallbladder removal?
Sometimes, especially with large or fatty meals. If fat remains hard to tolerate, bile salt support may be more effective. Discuss ongoing greasy stools with your clinician rather than escalating enzyme doses.
How to take it & ingredients
Suggested use: Take 1 to 2 capsules with each meal.
Active ingredients
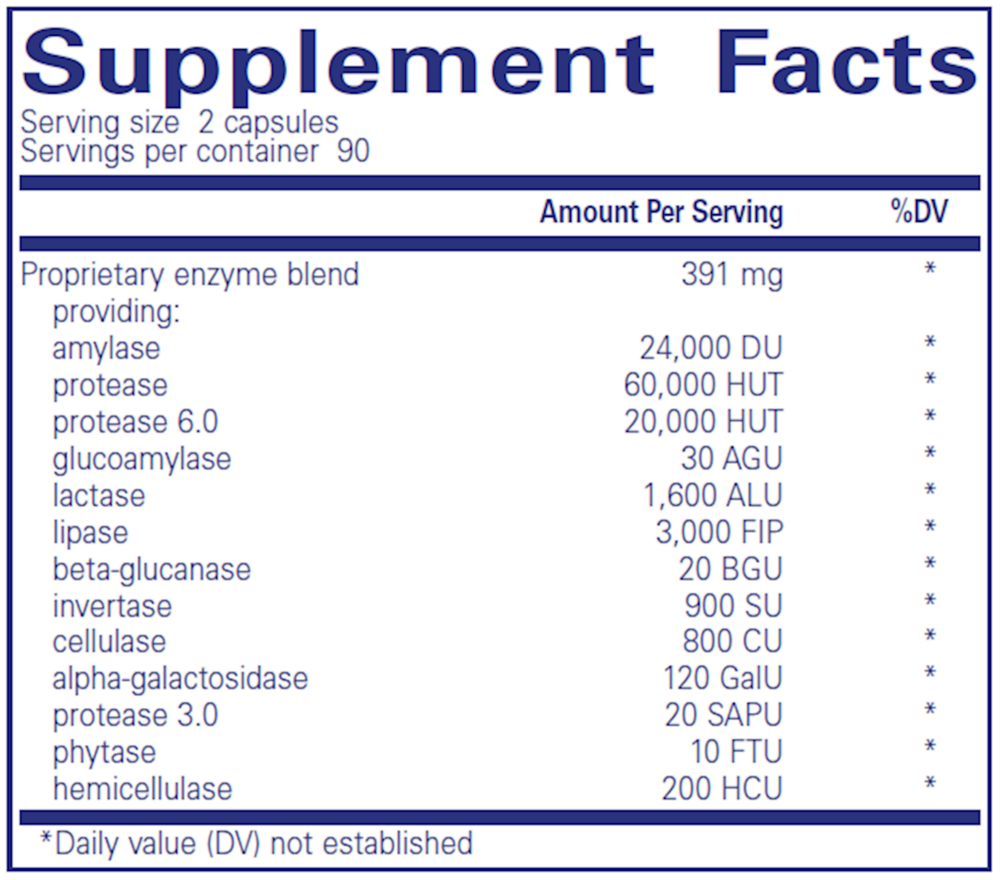
2 capsules per serving · 90 servings
▼
Proprietary Enzyme Blend
391 mg
Amylase
24000 DU
Protease
60000 HUT
Protease 6.0
20000 HUT
Glucoamylase
30 AGU
Lactase
1600 ALU
Lipase
3000 FIP
Beta-glucanase
20 BGU
Invertase
900 SU
Cellulase
800 CU
Alpha-galactosidase
120 GalU
Protease
3.0
3.0
3020 SAPU
Phytase
10 FTU
Hemicellulase
200 HCU
Other ingredients: Vegetarian capsule (cellulose, water), Ascorbyl palmitate, Hypoallergenic plant fiber (cellulose)
Certifications
Benefits
Warnings
Customers also considered

Thorne
Advanced Digestive Enzymes
180 capsules
$56.00extra 10% off with Subscribe & Save

Pure Encapsulations
Bromelain 2400 500mg
60 capsules
$40.00extra 20% off with Subscribe & Save

Ortho Molecular Products
DG Protect
60 capsules
$64.44extra 10% off with Subscribe & Save

Pure Encapsulations
Digestion GB
90 capsules
$36.50extra 21% off with Subscribe & Save