


Pure Encapsulations
Digestive Enzymes Ultra 391 mg by Pure Encapsulations
90 capsules · 45-day supply
Comprehensive Support for Healthy Digestion and Nutrient Absorption$38.00
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegetarian·Gluten Free·Egg Free·Artificial Preservative Free·Peanut Free·Wheat Free·
Pure Encapsulations Digestive Enzymes Ultra overview
If big, mixed meals leave you bloated or gassy, digestive enzymes can help at that meal, not weeks later. They’re a fit for high-protein dinners, high-fat restaurant food, bean-heavy or high-fiber bowls, and for lactose intolerance if the blend includes lactase. Older adults with lower natural enzyme output often notice clearer benefit. If you have true pancreatic insufficiency, confirm with Fecal Elastase-1 and use prescription pancrelipase; this blend is for functional bloating, not malabsorption with weight loss.
This broad-spectrum vegetarian blend supplies amylases for starch, proteases for protein, lipase for fat, lactase for milk sugar, and cellulase/hemicellulase plus alpha-galactosidase for plant fibers. By breaking food down before it reaches the colon, fewer leftovers feed gas-producing bacteria, so bloating and pressure ease. In healthy people, nutrient absorption improves only modestly; the real difference is meal comfort. For suspected lactose issues, a hydrogen breath test can confirm the diagnosis.
Take 1–2 capsules with the first bites of a meal. Enzymes work in the food bolus, so timing matters; taking them after you finish is less effective. Use them when you anticipate trouble meals and skip when you eat simply. Daily use is fine if you have predictable symptoms. Pairing with probiotics is okay, but they do different jobs, and enzymes do not replace a gluten-free diet if your celiac screen (tTG-IgA) is positive.
Skip self-treating with enzymes if you have unexplained weight loss, oily stools, persistent diarrhea, blood in stool, or anemia—see a clinician. Acute pancreatitis or chronic pancreatitis care should be guided by a specialist. People allergic to molds should note many enzymes are produced by Aspergillus species. Pregnancy and breastfeeding data are limited; use only if clearly helpful. Digestive enzymes won’t treat inflammatory bowel disease; monitor with calprotectin if that’s a concern.
Frequently asked questions
Do digestive enzymes help with bloating right away?
Often yes. If your bloating is from poor breakdown of carbs, fat, or protein, relief can show up at the very first meal. If symptoms don’t change after several tries, the cause may be unrelated to digestion and worth evaluating.
Should I take digestive enzymes with every meal?
Use them when you expect symptoms, like high-fat, high-protein, or high-fiber meals. Many people don’t need them for simple meals. Daily use is acceptable if you have consistent meal-triggered bloating and tolerate them well.
Can I take digestive enzymes with a PPI or antacid?
Yes. These enzymes are active across a range of pH levels. That said, long-term acid suppression can signal a separate issue; discuss persistent reflux with your clinician rather than relying on enzymes alone.
Are digestive enzymes good for lactose intolerance?
They can be, if the formula contains lactase. Look for lactase on the label and take it with the first bites of dairy. For a firm diagnosis, a hydrogen breath test can confirm lactose malabsorption.
Do digestive enzymes fix IBS or SIBO?
They don’t treat the root cause, but they can reduce meal-triggered gas if undigested carbs are the driver. For ongoing pain, altered bowel habits, or suspected SIBO, work with a clinician for testing and a full plan.
Can digestive enzymes cause side effects?
They’re usually well tolerated. Possible effects include mild nausea, loose stools, or stomach discomfort, often from taking them on an empty stomach or overdosing. Reduce the dose or reserve them for heavier meals.
Do digestive enzymes replace prescription pancrelipase?
No. For confirmed pancreatic insufficiency (low Fecal Elastase-1, weight loss, oily stools), prescription pancrelipase is standard. Over-the-counter blends are for functional bloating, not significant malabsorption.
How to take it & ingredients
Suggested use: Take 1 to 2 capsules with each meal.
Active ingredients
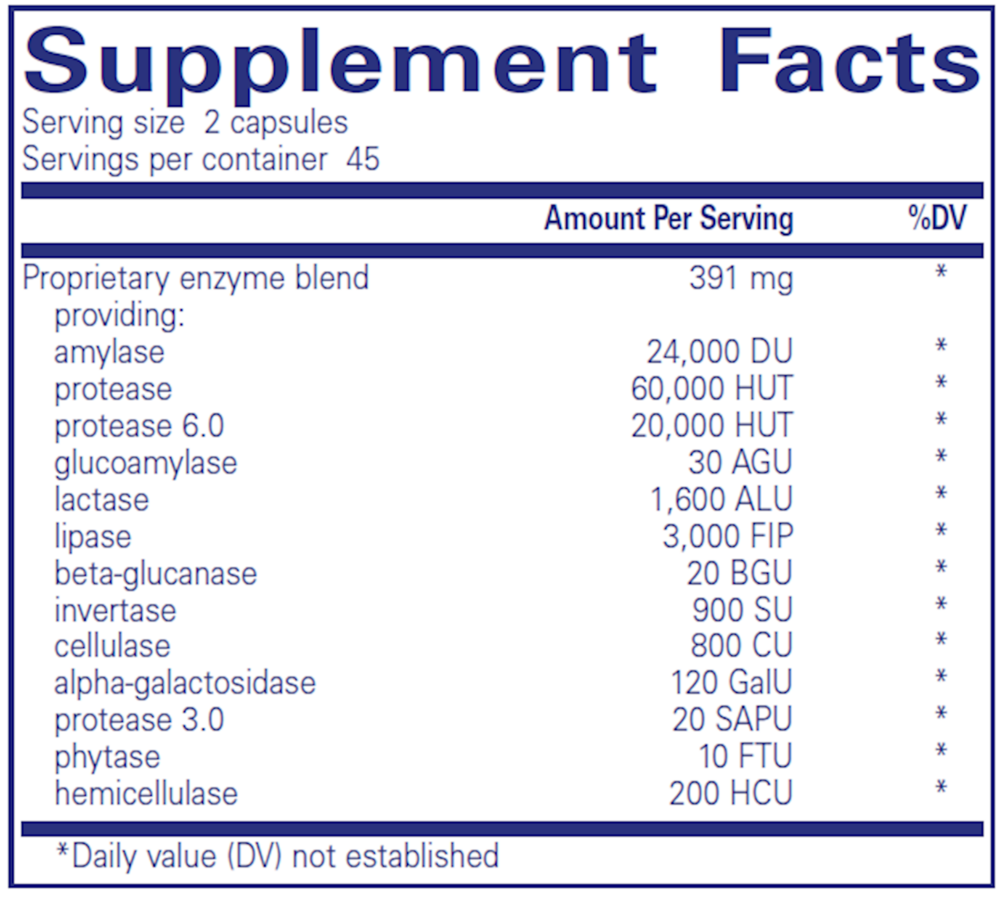
2 capsules per serving · 45 servings
▼
Proprietary Enzyme Blend
391 mg
Amylase
24000 DU
Protease
60000 HUT
Protease 6.0
20000 HUT
Glucoamylase
30 AGU
Lactase
1600 ALU
Lipase
3000 FIP
Beta-glucanase
20 BGU
Invertase
900 SU
Cellulase
800 CU
Alpha-galactosidase
120 GalU
Protease
3.0
3.0
3020 SAPU
Phytase
10 FTU
Hemicellulase
200 HCU
Other ingredients: Vegetarian capsule (cellulose, water), Ascorbyl palmitate, Hypoallergenic plant fiber (cellulose)
Certifications
Benefits
Warnings
Customers also considered

Thorne
Advanced Digestive Enzymes
180 capsules
$56.00extra 10% off with Subscribe & Save

Pure Encapsulations
Bromelain 2400 500mg
60 capsules
$40.00extra 20% off with Subscribe & Save

Ortho Molecular Products
DG Protect
60 capsules
$64.44extra 10% off with Subscribe & Save

Pure Encapsulations
Digestion GB
90 capsules
$36.50extra 21% off with Subscribe & Save