


Quicksilver Scientific
Nanoemulsified D3K2 by Quicksilver Scientific
50 milliliters
Essential Vitamins for Bone Health and Cardiovascular Support$XX.XX$55.99retail
This item is currently out of stockGet notified when this item is back in stock
20% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Gluten Free·Soy Free
Quicksilver Scientific Nanoemulsified D3K2 overview
If your Vitamin D, 25-Hydroxy is in the lower part of the normal range, this vitamin D3 K2 is a practical maintenance dose. It suits darker‑skinned adults, indoor workers, consistent sunscreen users, and anyone at northern latitudes. People with higher body weight often need more than 2,500 IU of vitamin D3 for repletion. If your level is meaningfully low, correct it under clinician guidance first, then use a vitamin D3 K2 maintenance plan.
Cholecalciferol (vitamin D3) is the form your skin makes from sunlight and raises blood levels more reliably than D2. It boosts calcium absorption from the gut and lowers parathyroid hormone (the signal that pulls calcium from bone). Vitamin K2 as MK‑7 activates proteins that move calcium into bone and keep it out of artery walls by carboxylating matrix Gla‑protein (a calcium‑binding brake in vessels). The nanoemulsion improves absorption and allows hold‑in‑mouth delivery for fast uptake.
Use 1 pump by mouth 1–2 times daily on an empty stomach, hold 30–90 seconds, then swallow. This provides 2,500 IU vitamin D3 plus 90 mcg K2 MK‑7 per pump, which is a maintenance‑level intake for most adults. If you are correcting deficiency, higher short‑term dosing is typical with follow‑up labs. Recheck Vitamin D, 25‑Hydroxy after 8–12 weeks. If you feel queasy on an empty stomach, take it 10–15 minutes before a meal with some fat.
Skip K2 if you take warfarin (a vitamin K–antagonist blood thinner) unless your prescriber plans INR monitoring. Direct oral anticoagulants like apixaban or rivaroxaban are not vitamin K–dependent, but still discuss changes. Avoid high‑dose vitamin D3 K2 if you have a history of high calcium, recurrent kidney stones, sarcoidosis, or primary hyperparathyroidism. Orlistat and bile acid binders reduce fat‑soluble vitamin absorption, so separate dosing by several hours.
Frequently asked questions
How long does vitamin D3 K2 take to raise my levels?
Most people see Vitamin D, 25-Hydroxy move meaningfully within 8–12 weeks. Repletion from true deficiency can take longer and often uses higher doses short term under clinician supervision.
Is 62.5 mcg of vitamin D3 a day a good dose?
62.5 mcg is 2,500 IU, a solid maintenance dose if your level is low‑normal. If your level is low, correction usually needs higher dosing for a few weeks, then stepping down to maintenance.
Can I take vitamin D3 K2 with calcium or magnesium?
Yes. Vitamin D3 K2 pairs well with calcium and magnesium for bone health. If you’re using a calcium supplement, split doses through the day to improve tolerance and absorption.
Does vitamin D3 K2 thin your blood?
No. Vitamin D3 does not thin blood. Vitamin K2 can interfere with warfarin, which relies on blocking vitamin K, so avoid K2 with warfarin unless your prescriber adjusts and monitors INR.
Morning or night for vitamin D3 K2?
Timing is flexible. Many take it in the morning on an empty stomach as directed. If you get mild nausea, take it shortly before a meal that includes some fat.
Is vitamin D3 K2 safe in pregnancy or breastfeeding?
Vitamin D3 is commonly used in pregnancy, guided by Vitamin D, 25-Hydroxy testing. K2 MK‑7 appears safe but data are limited; discuss dosing and labs with your obstetric clinician.
Is this vitamin D3 K2 vegan?
Most cholecalciferol (vitamin D3) is sourced from lanolin in sheep’s wool and is not vegan. If you need a vegan option, look for algae‑sourced D3 labeled as such.
What if I’m already on high-dose prescription vitamin D?
Don’t stack them. Finish your prescribed repletion plan, recheck Vitamin D, 25-Hydroxy, then consider transitioning to a maintenance product like vitamin D3 K2 if your clinician agrees.
How to take it & ingredients
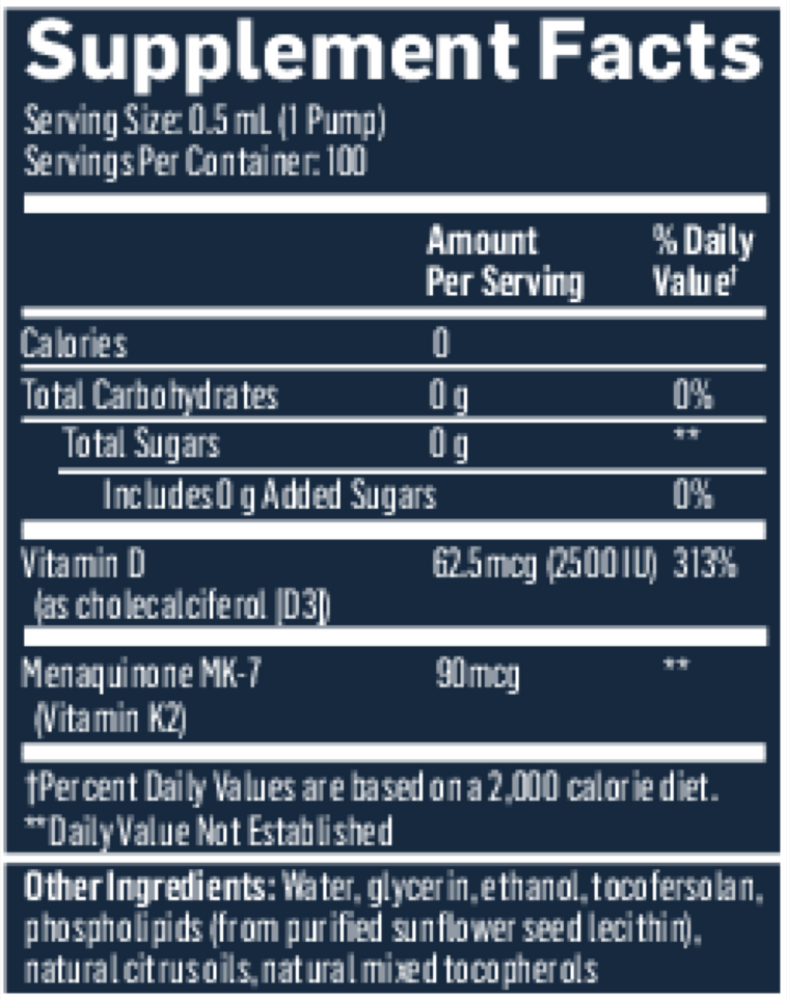
Suggested use: Take 1 pump by mouth 1 to 2 times daily. Hold in mouth 30 to 90 seconds before swallowing. Take on an empty stomach at least 10 minutes before meals or as directed by a healthcare professional.
Active ingredients
1 pump = 0.5 mL per serving
Vitamin D
Cholecalciferol (D3)
Cholecalciferol (D3)
62.5 mcg, 2500 IU
Vitamin K2
Menaquinone 7 (MK 7)
Menaquinone 7 (MK 7)
90 mcg
Other ingredients: Water, Glycerin, Ethanol, Tocofersolan, Highly Purified Phospholipids, Natural Mixed Tocopherols, Natural Citrus Oils
Certifications
Benefits
Warnings
Customers also considered

Ortho Molecular Products
K-FORCE
60 capsules
$XX.XX$60.33retail
Add to cart to see your price

Ortho Molecular Products
K-FORCE MAX
30 capsules
$XX.XX$44.79retail
Add to cart to see your price

Ortho Molecular Products
Liquid Vitamin D3 with K2
30 milliliters
$XX.XX$52.00retail
Add to cart to see your price

NBI
Osteo-K Minis
120 capsules
$XX.XX$65.99retail
Add to cart to see your price