


Thorne
Prenatal DHA by Thorne
60 gelcaps · 30-day supply
Essential Omega-3 Support for Expecting Mothers and Their Babies$30.00
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Dairy Free
Thorne Prenatal DHA overview
If you’re pregnant or breastfeeding and rarely eat fatty fish, prenatal DHA is one of the few supplements with clear payoff. This formula delivers 650 mg DHA plus 200 mg EPA per day, a range consistently used in pregnancy trials. It’s a strong fit if your Omega-3 Index is low, you’re carrying multiples, or you avoid seafood for taste, cost, or dietary reasons. It’s also practical if nausea makes fish unappealing, since softgels avoid odor. If your triglycerides are elevated, this amount helps nutrition but isn’t a high-dose omega-3 for lipid lowering.
DHA (docosahexaenoic acid) is the omega-3 your baby’s brain and eyes stockpile fastest in late pregnancy and early infancy. Supplementing raises DHA in your blood and breast milk within 2–4 weeks, which tracks with the Omega-3 Index test. EPA (eicosapentaenoic acid) tags along to improve DHA uptake and supports mom by tempering the rise in triglycerides that happens in pregnancy. Large trials show the biggest benefits for women who start with lower DHA, including fewer early preterm births. Claims around mood or immunity are mixed, so take omega-3s for fetal and infant development first.
Take two gelcaps with a meal, ideally one that contains some fat to improve omega-3 absorption. If you get fishy burps, take them right before the meal or split the dose morning and evening. Most see blood levels rise within 4–8 weeks; recheck your Omega-3 Index during the second trimester or early postpartum to confirm you’re in a good range. If you already eat fish several times weekly, one gelcap daily can serve as maintenance. For dedicated triglyceride reduction, higher-dose omega-3 products are more appropriate than a prenatal DHA.
Prenatal omega-3 from purified fish oil is low in mercury and generally well tolerated. If you’re on blood thinners like warfarin or a direct oral anticoagulant, talk to your clinician before adding fish oil and before any procedure. With fish or shellfish allergy, confirm the source and consider an algal DHA instead. Mild reflux is the most common side effect; taking with food solves it for most. This is not a replacement for prenatal vitamins, iodine, or choline, which address different needs measured by labs like Ferritin and Vitamin D, 25-Hydroxy.
Frequently asked questions
How much DHA should I take during pregnancy?
Most pregnancy studies use 200–1,000 mg DHA daily. This product provides 650 mg DHA plus 200 mg EPA, a clinically common target. If you already eat fatty fish several times weekly, you may need less; if your Omega-3 Index is low, this dose is appropriate.
How long does prenatal DHA take to work?
You’ll see blood omega-3 levels and breast milk DHA rise within 2–8 weeks. Many clinicians recheck the Omega-3 Index in the second trimester or early postpartum to confirm you’ve reached a healthy range for you.
Does fish oil thin your blood during pregnancy?
At typical prenatal DHA doses, bleeding risk is low. Even so, if you’re on anticoagulants or have a bleeding disorder, discuss dosing with your clinician and notify your obstetric team before procedures or delivery.
Is prenatal DHA safe from mercury and contaminants?
High-quality prenatal omega-3 uses purified fish oil with contaminant testing. That’s one advantage over eating large predatory fish. If you prefer a non-fish option, algal DHA is mercury-free and raises DHA similarly.
Can I take prenatal DHA with my prenatal vitamin?
Yes. Prenatal vitamins rarely contain enough DHA, so adding an omega-3 is common. Take DHA with a meal that has some fat to improve absorption, and keep taking iron, iodine, and choline as directed.
What if fish oil gives me burps or nausea?
Take capsules with your largest meal, split the dose, or refrigerate the softgels to reduce reflux. If symptoms persist, try an algal DHA or a smaller-per-capsule omega-3 taken more frequently.
Will prenatal DHA lower my triglycerides?
It can blunt the normal pregnancy rise in triglycerides, but meaningful lowering usually needs higher total EPA+DHA (2–4 grams daily). Use a dedicated high-dose omega-3 for lipids, and track with a lipid panel.
How to take it & ingredients
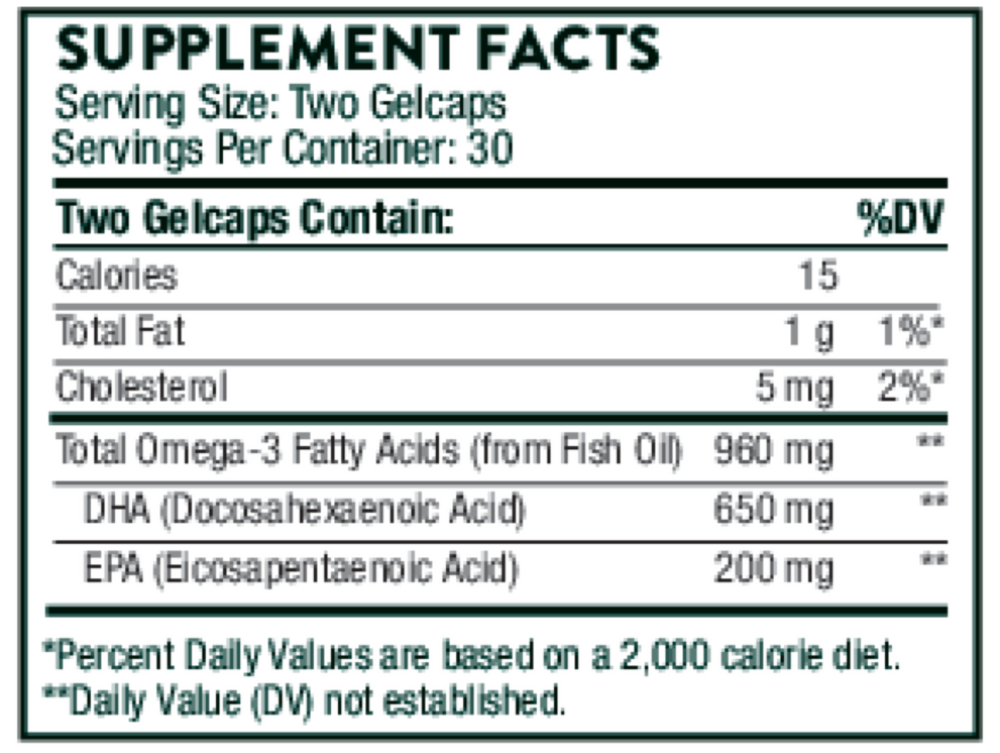
Suggested use: Take 2 gelcaps daily or as recommended by your health-care practitioner.
Active ingredients
2 gelcaps per serving · 30 servings
Total Omega-3 Fatty Acids
960 mg
Docosahexaenoic Acid (DHA)
650 mg
Eicosapentaenoic Acid (EPA)
200 mg
Other ingredients: Antioxidant Blend (Vitamin E (mixed tocopherols) and Rosemary Extract), Gelatin (Bovine), Glycerin (Vegetable Source), Mint Flavor, Purified Water Gelcap
Certifications
Benefits
Warnings
Customers also considered

Thorne
Advanced DHA
60 gelcaps
$30.00extra 10% off with Subscribe & Save

Garden of Life
Dr. Formulated Advanced Omega
60 softgels
$31.99extra 19% off with Subscribe & Save
Garden of Life
Dr. Formulated DHA 1g
30 softgels
$31.99extra 19% off with Subscribe & Save
Garden of Life
Dr. Formulated Prenatal DHA
30 softgels
$29.99extra 20% off with Subscribe & Save