


Thorne
Super EPA Pro 1500 mg by Thorne
120 gelcaps · 60-day supply
Premium Omega-3 Support for Heart, Brain, and Joint Health$93.00
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Dairy Free·Milk Free
Thorne Super EPA Pro overview
If your triglycerides are elevated and you want a non-statin add‑on with measurable impact, a high‑EPA fish oil fits. It also suits those with a low Omega‑3 Index who rarely eat fatty fish, and people tracking inflammation who see higher hs‑CRP (a blood marker of systemic inflammation). Vegans and strict vegetarians should choose an algal omega‑3 instead. For general maintenance, this potency is more than you need; it is intended for targeted triglyceride reduction.
EPA and DHA are long‑chain omega‑3 fats from fish oil. They reduce how much fat your liver exports in VLDL particles (the carriers that show up on a lipid panel as triglycerides), and they nudge cells to burn fatty acids for energy faster. Most responders see triglycerides drop 20–30% within 4 to 12 weeks at prescription‑level intakes. EPA‑heavy formulations tend to lower triglycerides without the small LDL‑cholesterol bump seen in some people with DHA‑heavy oils. Modest reductions in hs‑CRP occur in some, but not all, patients.
The suggested use is two gelcaps twice daily. Because these are ethyl ester forms, take them with a meal that contains fat to improve absorption and limit fishy burps. Splitting the dose morning and evening keeps blood levels steadier. If you are only maintaining an already good Omega‑3 Index, a lower total daily omega‑3 may be sufficient; this regimen is a therapeutic dose for high triglycerides.
If you use blood thinners like warfarin, apixaban, rivaroxaban, or clopidogrel, talk with your clinician and consider checking a baseline and follow‑up for bruising or bleeding. Stop 3–5 days before planned surgery unless your surgeon advises otherwise. If you have a history of irregular heartbeat, especially atrial fibrillation (episodes of a racing, uneven pulse), discuss high‑dose omega‑3 with your cardiologist. Avoid if you have a fish allergy.
Frequently asked questions
How long does fish oil take to lower triglycerides?
You typically see changes on a lipid panel within 4 to 12 weeks. The response depends on dose, baseline diet, and adherence. Retest triglycerides after 8 to 12 weeks and continue if you are a responder.
Does fish oil thin your blood?
At typical doses it has a mild anti‑platelet effect, which can slightly increase bruising in some people. Clinically meaningful bleeding is uncommon, but use caution with warfarin, apixaban, rivaroxaban, or clopidogrel and before surgery.
Is EPA or DHA better for high triglycerides?
EPA‑dominant fish oil is preferred for triglyceride lowering because it reduces liver fat export and tends not to nudge LDL cholesterol up. DHA‑heavy oils can lower triglycerides too, but may raise LDL cholesterol slightly in some people.
Will fish oil raise my LDL cholesterol?
EPA‑dominant formulas rarely raise LDL cholesterol. DHA‑dominant or mixed oils can raise LDL cholesterol modestly in some. If this is a concern, favor high‑EPA products and recheck a full lipid panel after 8 to 12 weeks.
Can I take fish oil with statins or fibrates?
Yes. Omega‑3s pair well with statins and with fibrates when triglycerides are high. Many clinicians use them together. Monitor your lipid panel, and let your prescriber know you added fish oil.
What labs should I check on fish oil?
Track Triglycerides, non‑HDL cholesterol, and the Omega‑3 Index. If you are interested in inflammation, include hs‑CRP. Recheck after 8 to 12 weeks to confirm your response.
How do I reduce fishy burps from fish oil?
Take capsules with a fat‑containing meal, split the dose, and consider keeping them in the freezer. These steps slow dissolution in the stomach and usually eliminate reflux.
Is this fish oil good in pregnancy?
Fish oil is generally safe, but pregnancy prioritizes DHA for fetal brain and eye development. This product is EPA‑heavy, so consider a DHA‑rich prenatal omega‑3 after discussing with your obstetric clinician.
How to take it & ingredients
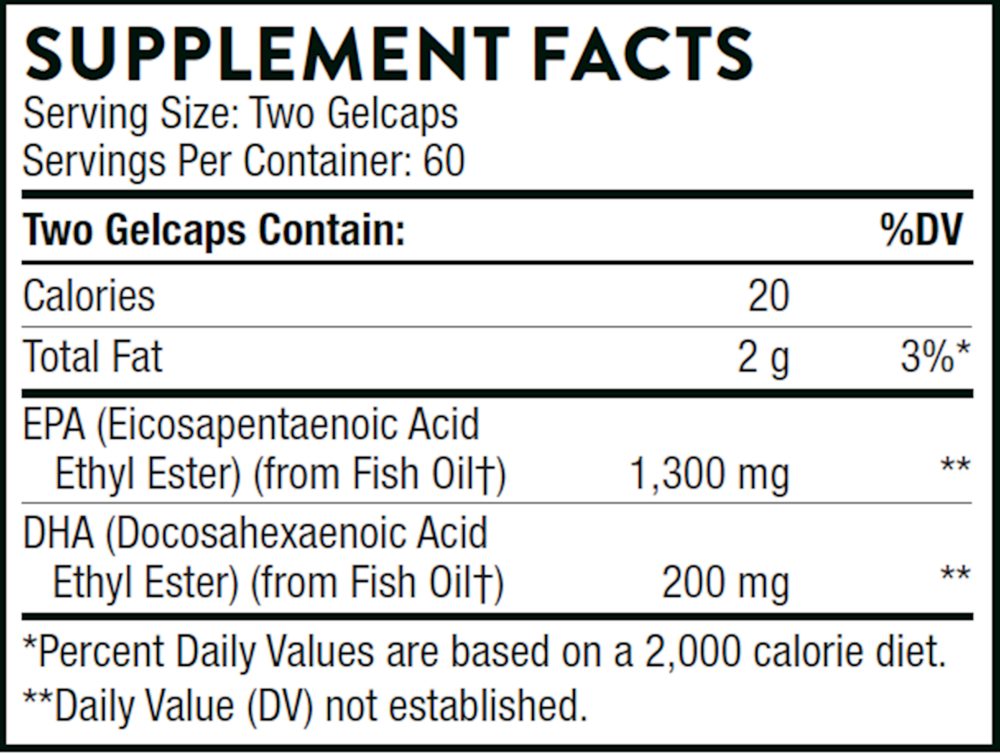
Suggested use: Take 2 gelcaps two times daily or as recommended by your health professional.
Active ingredients
2 gelcaps per serving · 60 servings
▼
Total Omega-3 Fatty Acids
From Fish Oil
From Fish Oil
1500 mg
EPA (Eicosapentaenoic Acid (Ethyl Ester)
From Fish Oil
From Fish Oil
1300 mg
DHA (Docosahexaenoic Acid Ethyl Ester)
From Fish Oil
From Fish Oil
200 mg
Other ingredients: Gelatin (Bovine), Purified Water, Glycerin (Vegetable Source)
Certifications
Benefits
Warnings
Customers also considered

Thorne
Advanced DHA
60 gelcaps
$30.00extra 10% off with Subscribe & Save

Garden of Life
Dr. Formulated Advanced Omega
60 softgels
$31.99extra 19% off with Subscribe & Save
Garden of Life
Dr. Formulated DHA 1g
30 softgels
$31.99extra 19% off with Subscribe & Save
Garden of Life
Dr. Formulated Prenatal DHA
30 softgels
$29.99extra 20% off with Subscribe & Save