

Ortho Molecular Products
CDG EstroDIM by Ortho Molecular Products
60 capsules · 30-day supply
Support Hormonal Balance with a Powerful Blend of Nutrients$103.73
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Corn Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products CDG EstroDIM overview
This is for adults looking to improve estrogen metabolism with DIM and calcium D‑glucarate, especially if labs like Estradiol and Estrone run high-normal and symptoms track with your cycle (breast tenderness, heavy periods, PMS). It also fits men on testosterone therapy whose Estradiol creeps up. If your urinary estrogen metabolites (the 2‑OH, 4‑OH, 16‑OH forms measured on advanced urine testing) are unfavorable, this combo is a practical first step.
DIM from cruciferous vegetables nudges estrogen toward 2‑hydroxylation, a set of breakdown products linked with fewer growth signals in estrogen‑sensitive tissues. Indole‑3‑carbinol (I3C) converts to DIM in the stomach and adds the same push. Calcium D‑glucarate supports glucuronidation, the liver’s “tag and ship out” step, and limits beta‑glucuronidase in the gut (an enzyme that can untag and recirculate hormones), so estrogens exit in bile and stool. Vitamin E provides antioxidant cover for these reactions. Evidence is strongest for shifting lab biomarkers, not for hard outcomes like cancer risk.
Take two capsules daily with food, ideally with some fat for absorption and to reduce nausea. Most people see shifts in urinary estrogen metabolites within 4–8 weeks, with symptom changes over 1–3 cycles. Track Estradiol, Estrone, and urinary metabolites to gauge effect. This is a meaningful, not extreme, dose; if your pattern is severely abnormal, coordinate a higher‑touch plan with your clinician.
DIM and I3C can induce liver enzymes (like CYP1A2/3A4), which can lower levels of some drugs. Be cautious with oral contraceptives, hormone therapy, benzodiazepines, calcium‑channel blockers, certain antidepressants, and statins—get personalized advice. Calcium D‑glucarate can also increase clearance of medications processed by the liver. Skip if pregnant, trying to conceive, or breastfeeding. If you have very low estrogen (missed periods, underweight), this can worsen symptoms. Cancer survivors on aromatase inhibitors or SERMs should only use with their oncologist.
Frequently asked questions
What does DIM do for estrogen?
DIM shifts estrogen breakdown toward 2‑hydroxylation (metabolites linked to less tissue growth) and away from 16‑hydroxylation. In practice, people see improved urinary estrogen metabolite patterns and steadier cycle symptoms when it’s a good fit.
How long does DIM take to work?
Biomarker changes often show up within 4–8 weeks on urine metabolite testing. Symptom changes typically track over 1–3 menstrual cycles. Give it at least two full cycles before judging response, and recheck labs to confirm it’s doing what you want.
Can I take DIM with birth control?
Use caution. DIM and I3C can increase liver enzyme activity, which could reduce hormone levels from oral contraceptives. If you choose to take them together, discuss with your clinician and consider backup contraception until you know your response.
Is DIM safe for men?
Yes for the right use case. Men with high Estradiol on testosterone therapy sometimes use DIM to improve estrogen metabolism. Monitor Estradiol, Sex Hormone–Binding Globulin (SHBG), and symptoms, and avoid if you already run low on estrogen.
Should I take DIM with food or on an empty stomach?
Take it with food, preferably containing some fat. That improves absorption and reduces common side effects like nausea or reflux. Splitting the dose across breakfast and dinner can help if your stomach is sensitive.
What labs should I track while using DIM?
Track Estradiol and Estrone on bloodwork and, if available, urinary estrogen metabolites (2‑OH, 4‑OH, 16‑OH pathways). If you take other medications, periodic liver enzymes (ALT, AST) can be useful to ensure you’re tolerating the regimen.
What side effects can DIM or I3C cause?
Most are mild: nausea, changes in stool, headache, or darkened urine odor. Taking with food usually helps. If you feel jittery or notice drug effects changing (like sedation wearing off faster), speak with your clinician about interactions.
Can I use DIM if I’m trying to get pregnant?
No. Avoid during preconception, pregnancy, and breastfeeding. These compounds modify estrogen pathways, which isn’t appropriate when you’re aiming for implantation, supporting a pregnancy, or lactating.
How to take it & ingredients
Suggested use: 2 capsules per day or as recommended by your health care professional.
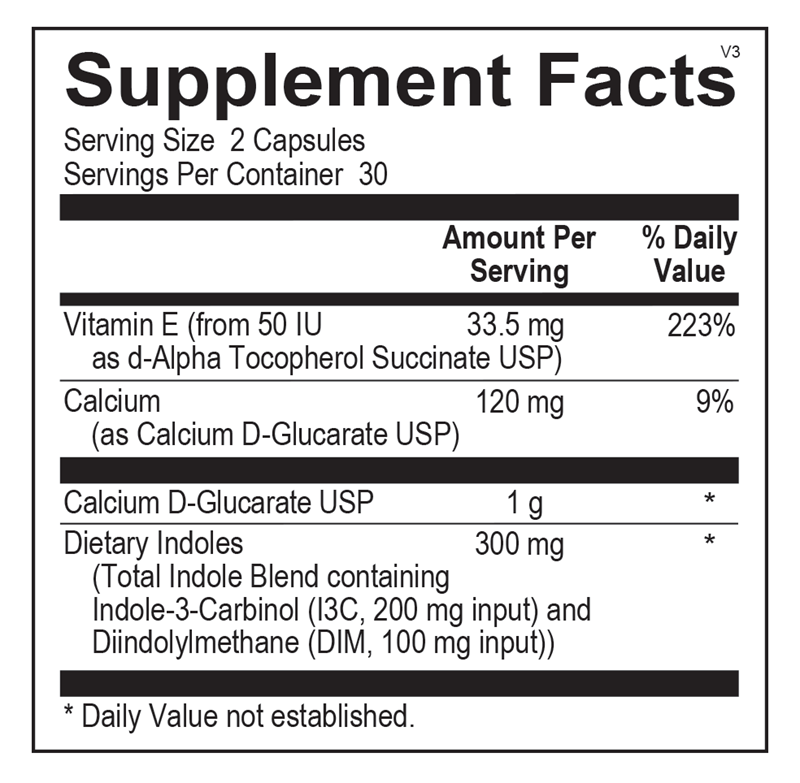
Active ingredients
2 capsules per serving · 30 servings
Vitamin E
As d-Alpha Tocopherol Succinate USP
As d-Alpha Tocopherol Succinate USP
33.5 mg
Calcium
As Calcium D-Glucarate USP
As Calcium D-Glucarate USP
120 mg
Calcium D-Glucarate
USP
USP
1000 mg
Indole-3-Carbinol (I3C)
200 mg
Diindolylmethane (DIM)
100 mg
Other ingredients: Hypromellose (Natural Vegetable Capsules), Magnesium Stearate, Silicon Dioxide, Stearic Acid
Certifications
Benefits
Warnings
Customers also considered
Ortho Molecular Products
Balance
60 capsules
$47.90extra 10% off with Subscribe & Save

Vitanica
Black Cohosh
60 capsules
$17.99extra 22% off with Subscribe & Save

Pure Encapsulations
Black Cohosh 2.5
120 capsules
$53.00extra 21% off with Subscribe & Save

Vitanica
BreastBlend™
90 capsules
$51.99extra 19% off with Subscribe & Save