

Ortho Molecular Products
CoQ-10 300 MG by Ortho Molecular Products
60 softgels · 60-day supply
High-Strength CoQ10 Antioxidant for Cardiovascular and Cellular Energy Support$108.28
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products CoQ-10 300 MG overview
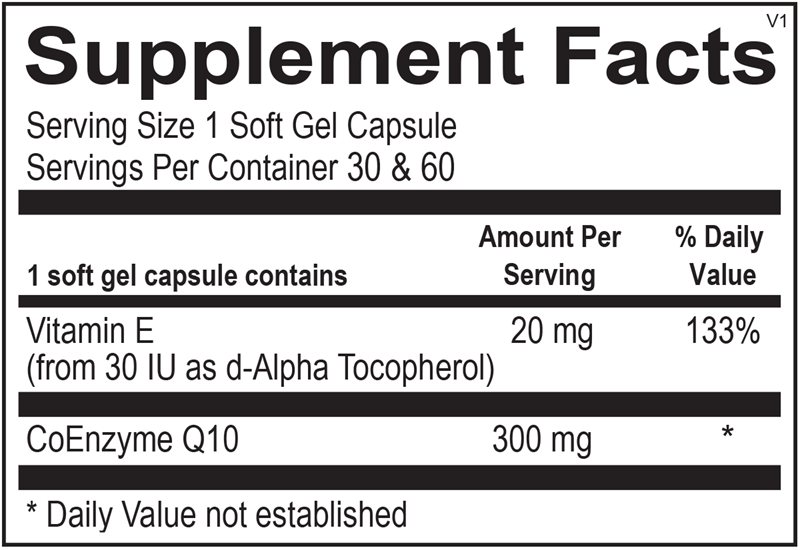
This formula suits adults who want a high-strength daily dose of CoQ-10 alongside natural vitamin E. Each softgel provides 300 mg of CoQ-10, an antioxidant nutrient the body uses in cellular energy production, paired with 20 mg of vitamin E from d-Alpha Tocopherol. It is a once-daily, oil-based softgel intended as part of a routine focused on cardiovascular support and antioxidant intake.
CoQ-10 (Coenzyme Q10) is a lipid-soluble antioxidant found in every cell. It participates in the electron transport chain inside mitochondria, the cellular structures that produce ATP, the chemical form of energy the body uses. It also acts as an antioxidant, helping protect lipids in cell membranes from oxidative damage. The added natural vitamin E (d-Alpha Tocopherol) is a fat-soluble antioxidant that supports antioxidant activity in the same lipid environment, which is why Ortho Molecular pairs the two in this oil-based softgel.
Take one softgel per day, ideally with a meal that contains some dietary fat, since CoQ-10 is fat-soluble and absorption improves alongside food. Morning or midday tends to fit most routines. Use as directed by your health care professional.
If you take prescription medications, are pregnant or breastfeeding, or are managing a health condition with a clinician, talk to your care team before starting and review the warnings below.
Frequently asked questions
How much CoQ-10 and vitamin E does each softgel provide?
Each softgel contains 300 mg of CoQ-10 (Coenzyme Q10) and 20 mg of vitamin E from d-Alpha Tocopherol (133% of the Daily Value). One softgel is the daily serving.
What form of CoQ-10 does this use?
This formula uses CoQ-10 in an oil-based softgel. The two main commercially available forms of CoQ-10 are ubiquinone (the oxidized form) and ubiquinol (the reduced form). Ortho Molecular does not label this product as ubiquinol on the supplement facts panel, so it follows the standard CoQ-10 format.
Should I take CoQ-10 with food?
Yes. CoQ-10 is fat-soluble, so taking the softgel with a meal that contains some dietary fat can support absorption. Many adults take it at breakfast or lunch.
When during the day should I take it?
Morning or midday with a meal tends to fit most routines. Some adults find later-evening dosing affects sleep, so earlier in the day is a reasonable default.
Why is there vitamin E in a CoQ-10 supplement?
Vitamin E is a fat-soluble antioxidant. Including 20 mg of natural d-Alpha Tocopherol in the same oil-based softgel supports antioxidant activity in the same lipid environment where CoQ-10 functions.
Is the vitamin E in this product natural or synthetic?
It is natural d-Alpha Tocopherol, the naturally occurring stereoisomer of vitamin E, listed on the supplement facts panel as 20 mg from 30 IU as d-Alpha Tocopherol.
How to take it & ingredients
Suggested use: Take 1 soft gel capsule per day or as recommended by your health care professional.
Active ingredients
1 softgel per serving · 60 servings
Vitamin E
D-Alpha Tocopherol
D-Alpha Tocopherol
20 mg
Coenzyme Q10
300 mg
Other ingredients: D-Limonene Oil, Gelatin, Glycerin, Purified Water, Mixed Tocopherols, Red Radish Powder, Carob Extract Concentrate, Caramel Liquid, Medium Chain Triglycerides
Certifications
Benefits
Warnings
Customers also considered

Jarrow Formulas
Co-Q10 200mg
60 capsules
$41.99extra 19% off with Subscribe & Save

Ortho Molecular Products
CoQ-10
30 softgels
$51.67extra 10% off with Subscribe & Save

Thorne
CoQ10
60 gelcaps
$53.00extra 10% off with Subscribe & Save

Thorne
Heart Health Complex
90 capsules
$43.00extra 10% off with Subscribe & Save