

Ortho Molecular Products
EstroDIM® by Ortho Molecular Products
60 capsules · 60-day supply
Support Hormonal Balance with DIM and Vitamin E for Women's Health$67.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products EstroDIM® overview
If your Estradiol is normal or high and you feel “estrogen-heavy” (PMS breast tenderness, cyclical acne, water retention), a DIM supplement is a practical first step. It fits perimenopausal adults with higher estrogen relative to Progesterone, and those with high-normal Estradiol on labs who prefer a non-hormone option. If your estrogen is already low, or you’re on prescription hormones, get guidance before using DIM.
DIM (3,3'-diindolylmethane) is the concentrated compound from cruciferous vegetables that nudges estrogen toward “cleaner” breakdown products. It increases 2-hydroxylation (a pathway that produces less stimulatory metabolites) and reduces 16-hydroxylation (a pathway linked to tissue overstimulation). You can track this with urinary Estrogen Metabolites testing. Unlike I3C (indole-3-carbinol), DIM is the direct active, so the effect is more predictable at a given dose.
One capsule daily with a meal that contains fat is ideal, because DIM is fat-soluble. The 300 mg dose here is at the higher end; many clinicians start at 100–200 mg and titrate. Expect shifts in urinary Estrogen Metabolites within 4 to 8 weeks and symptom changes over 1–2 cycles. Vitamin E (33.5 mg) is included for stability and absorption support.
Avoid during pregnancy or while trying to conceive, and skip while breastfeeding. If your Estradiol is low, DIM can worsen hot flashes or vaginal dryness. Use caution with oral contraceptives or hormone therapy; DIM can induce liver enzymes (CYP3A), which could reduce hormone levels. Oncology patients on tamoxifen or aromatase inhibitors should only use DIM under their oncologist.
Because DIM can increase drug metabolism in the liver, review it with your clinician if you take medications processed by CYP3A (examples include some statins, calcium-channel blockers, and anti-seizure drugs). Track Estradiol, Progesterone, and Sex Hormone Binding Globulin (SHBG) if you’re adjusting hormones. Mild nausea or darker urine can occur and are usually self-limited.
Frequently asked questions
What does a DIM supplement actually do?
DIM shifts how your body breaks down estrogen toward less stimulatory metabolites. People use it for PMS breast tenderness, cyclical acne, or feeling “estrogen-heavy.” It doesn’t add or remove estrogen directly; it changes the balance of downstream metabolites you can measure in urine.
How long does DIM take to work?
Most see changes in urinary Estrogen Metabolites within 4–8 weeks and symptom changes over 1–2 menstrual cycles. If nothing shifts by 8 weeks, reassess dose, adherence with food, and whether low estrogen or another driver is the issue.
Can I take DIM with birth control pills?
Be cautious. DIM can induce liver enzymes that may lower hormone levels, which could reduce pill effectiveness. If you choose to use DIM, discuss it with your prescriber and use backup contraception until you’ve reviewed risks.
Is DIM safe during pregnancy or breastfeeding?
No. There’s insufficient safety data in pregnancy or lactation, and altering estrogen metabolism is not appropriate when hormones are supporting fetal or infant development. Avoid while trying to conceive as well.
Should I take DIM or indole-3-carbinol (I3C)?
DIM is the direct active compound; I3C must convert to DIM in the stomach, and the yield varies. If you want predictable dosing, use DIM. Some clinicians use I3C short term for broader effects, but DIM is simpler to standardize.
Can men take DIM for high estrogen or gynecomastia?
Yes, with labs. Men with high Estradiol or low Testosterone-to-Estradiol ratio sometimes use DIM to improve estrogen metabolism. Check Estradiol, Testosterone, and SHBG first, and recheck after 4–8 weeks to avoid overshooting.
What are common DIM side effects?
Mild nausea, headache, or darker urine can occur, especially when starting or taking it on an empty stomach. Taking it with a meal that contains fat usually fixes this. If hot flashes or dryness worsen, your estrogen may be low—pause and reassess.
Does DIM affect other medications?
Potentially. DIM can increase liver enzyme activity (CYP3A), which may lower levels of certain drugs such as some statins, calcium-channel blockers, and anti-seizure meds. Review your list with a clinician before starting.
How to take it & ingredients
Suggested use: 1 capsule per day or as recommended by your health care professional.
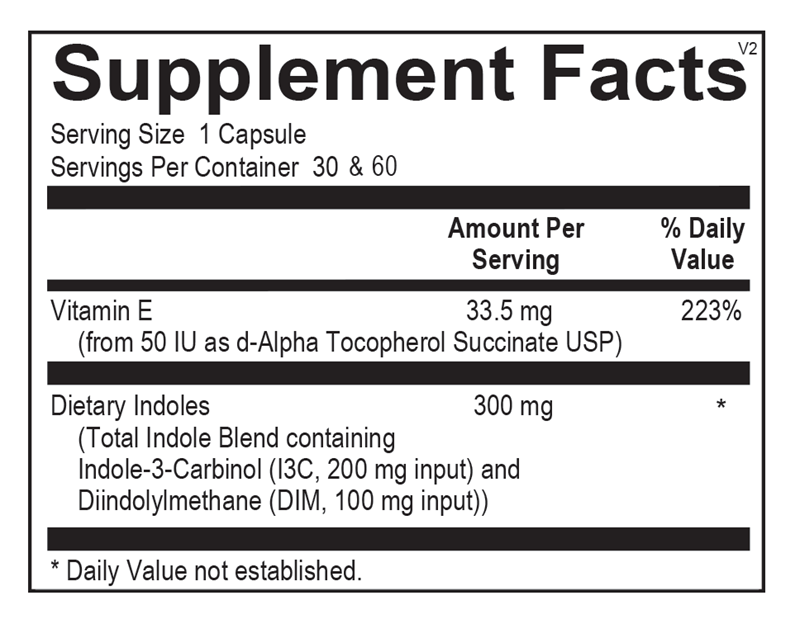
Active ingredients
1 capsule per serving · 60 servings
Vitamin E
33.5 mg
3,3'-Diindolylmethane (DIM)
300 mg
Certifications
Benefits
Warnings
Customers also considered
Ortho Molecular Products
Balance
60 capsules
$47.90extra 10% off with Subscribe & Save

Vitanica
Black Cohosh
60 capsules
$17.99extra 22% off with Subscribe & Save

Pure Encapsulations
Black Cohosh 2.5
120 capsules
$53.00extra 21% off with Subscribe & Save

Vitanica
BreastBlend™
90 capsules
$51.99extra 19% off with Subscribe & Save