

Ortho Molecular Products
Pregnenolone 10 mg by Ortho Molecular Products
100 tablets · 100-day supply
Support Hormonal Balance and Vitality with Pregnenolone$31.47
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Wheat Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Pregnenolone overview
This is for adults exploring a pregnenolone supplement after seeing low or low-normal adrenal-and-gonadal markers on labs. In practice, that means you and your clinician are tracking Cortisol (AM serum or salivary cortisol), DHEA-S (the stable blood form of DHEA), and often Progesterone, Estradiol, and Total Testosterone. The 10 mg dose suits cautious, lab-guided trials, especially if you’re sensitive to stimulants, have sleep fragility, or are already using DHEA or progesterone and want a gentle upstream nudge.
Pregnenolone is the steroid precursor your body makes from cholesterol in mitochondria, and it’s the starting point for progesterone, DHEA, cortisol, and downstream sex hormones. Because it sits upstream, small changes can echo across multiple hormones, including the HPA axis (the brain-to-adrenal stress control system). It’s also a neurosteroid, meaning it modulates brain receptors that influence alertness and mood. Human data are limited, so expectations should stay modest and anchored to labs and how you feel.
Start with one tablet in the morning, with or without food, since taking it late can disrupt sleep. Recheck Cortisol and DHEA-S within 4 to 8 weeks, and adjust only if labs and symptoms align. If you’ve never used hormone-related supplements, stay at 10 mg for a full month before considering a change. If you need larger shifts, clinicians often consider DHEA or progesterone directly rather than pushing pregnenolone higher.
Avoid if pregnant, trying to conceive, or breastfeeding. Skip if you have a history of hormone-sensitive cancers, uncontrolled endometriosis, or prostate issues, unless your specialist agrees and monitors labs. Use caution with steroid medications (like prednisone), thyroid dose changes, or if you’ve had acne, irritability, or insomnia on DHEA or testosterone—those can signal sensitivity to upstream hormones. Any unexplained mood shift, palpitations, or sleep disruption is a cue to stop and recheck labs.
Frequently asked questions
What does a pregnenolone supplement do?
It provides an upstream steroid precursor that can slightly influence progesterone, DHEA, and cortisol pathways. Effects are individualized, so track Cortisol and DHEA-S and judge by both labs and how you feel.
How long does pregnenolone take to work?
Most lab and symptom changes, if they occur, show within 4 to 8 weeks. Recheck Cortisol and DHEA-S then. If nothing moves, consider stopping or shifting to targeted hormones with your clinician.
Is 10 mg a low dose of pregnenolone?
Yes. Ten milligrams is a cautious, physiologic dose. It’s appropriate for first-time trials or sensitive users. Larger shifts are usually handled with DHEA or progesterone directly rather than pushing pregnenolone high.
When should I take pregnenolone, morning or night?
Morning is best. Pregnenolone can feel stimulating for some, and evening dosing can disrupt sleep. Take it with or without food based on your stomach comfort.
What are common side effects of pregnenolone?
Possible effects include restlessness, insomnia, irritability, acne or oily skin, and headache. These suggest you’re hormonally sensitive or the dose is too high. Stop and recheck labs if you notice these.
Can I take pregnenolone with DHEA or progesterone?
You can, but do it intentionally and monitor. Combining can overshoot. Track DHEA-S, Progesterone, and Cortisol, and adjust only if labs and symptoms point the same way.
Is pregnenolone safe for women with PCOS or men with prostate issues?
Be cautious. Because it sits upstream of multiple hormones, it can aggravate acne, hair growth, cycles, or prostate symptoms. Only use with clinician guidance and close lab follow-up.
Do I need labs before starting pregnenolone?
Strongly recommended. Baseline Cortisol and DHEA-S set a reference point, and repeating them in 4–8 weeks shows whether the dose helps or should be stopped.
How to take it & ingredients
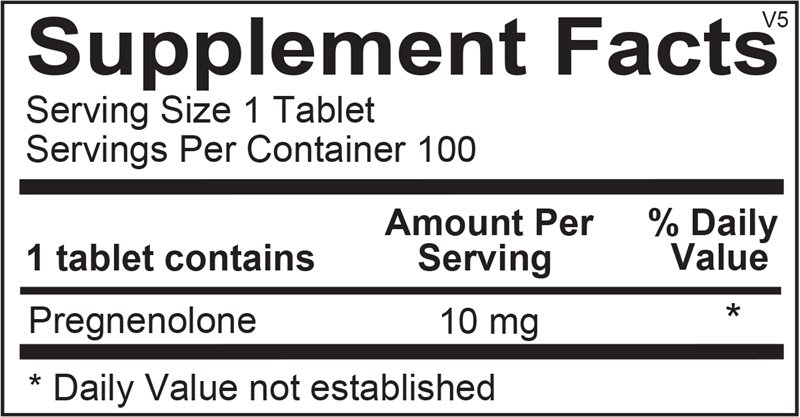
Suggested use: 1 or more tablets per day or as recommended by your health care professional.
Active ingredients
1 tablet per serving · 100 servings
Pregnenolone
10 mg
Certifications
Benefits
Warnings
Customers also considered
Ortho Molecular Products
Balance
60 capsules
$47.90extra 10% off with Subscribe & Save

Vitanica
Black Cohosh
60 capsules
$17.99extra 22% off with Subscribe & Save

Pure Encapsulations
Black Cohosh 2.5
120 capsules
$53.00extra 21% off with Subscribe & Save

Vitanica
BreastBlend™
90 capsules
$51.99extra 19% off with Subscribe & Save